Mitral valve aneurysm is a rare condition usually associated with aortic valve endocarditis. The mechanism, poorly understood, generally includes a regurgitant infectious flow originating from the aortic valve, direct contact with vegetation and direct propagation, through adjacent structures, such as the mitro-aortic intervalvular fibrous body. This report details the case of a 56-year-old patient followed for severe bicuspid aortic insufficiency of the aortic valve for 4 months and admitted to heart failure due to infectious endocarditis with a fatal outcome. Physical examination revealed aortic and mitral insufficiency syndrome and congestive heart failure. Transthoracic echocardiography revealed type 1 L-R bicuspid heart disease and leaking polyvalvulopathy with severe eccentric aortic and severe mitral regurgitation. The aortic and mitral valves were the seat of the vegetations. The mitral valve was the seat on its atrial side of a contained aneurysmal sac with thrombosed hyperechogenicity. Blood cultures were positive for streptococci and probabilistic dual antibiotic therapy was started. The patient was unable to benefit from surgical treatment. However, the patient died following complications such as ischemic stroke and septic shock. A necropsy was not done.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Anterior mitral valve aneurysm (AVM) is a rare entity. It is defined as a protuberance located on the atrial side of the mitral leaflet presenting systolic expansion and diastolic collapse
[1]
Tariq, M., Zahid, I., Sami, S. Rare aneurysm of anterior mitral valve leaflet-a case report. J Cardiothorac Surg. 2019; 14: 204.
. It is frequently associated with infective endocarditis in aortic insufficiency
[2]
Vilacosta, I., San Román, J. A., Sarriá, C. Clinical, anatomic, and echocardiographic characteristics of aneurysms of the mitral valve. Am J Cardiol. 1999; 84(1): 110-3.
, connective tissue defect or degeneration of valve tissue have also been described
[5]
Guler, A., Karabay Can, Y., Gursoy Ozan, M. Clinical and echocardiographic evaluation of mitral valve aneurysms: a retrospective, single center study. Int J Cardiovasc Imaging. 2014; 30: 535-41.
. This report presents the case of an aneurysm of the anterior mitral valve due to infective endocarditis in a bicuspid aortic joint with fatal outcome.
2. Observation
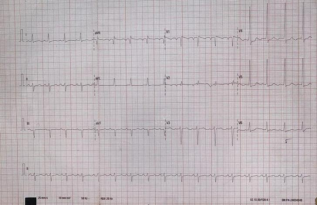
56-year-old patient, followed for 4 months for severe aortic insufficiency with left ventricular systolic dysfunction. Two weeks before admission, the patient reported symptoms consisting of onset of dyspnea and progressive worsening, admitting an orthopneic component, a deterioration in general condition and fever. Upon admission, the patient exhibited tachycardia at 107/min, a normal temperature of 36.2°C, a blood pressure of 113/49 mm Hg and an SpO2 of 99% on ambiant air. Physical examination revealed clear consciousness with a Glasgow Coma Scale score of 15/15, a fairly good general condition, a displaced and diffuse apex beat to the left at the anterior axillary line, regular heart sounds with a soft, blowing diastolic murmur at the left sternal border, a holosystolic murmur at the mitral area with a jet-like quality, peripheral signs of aortic insufficiency (bounding pulses, hyperpulsatility of the neck vessels, widened pulse pressure...), clear lung fields with well-perceived vesicular breath sounds, and signs of global heart failure (NYHA stage 4 dyspnea with an orthopneic component, spontaneous jugular vein distension, congestive liver, and mild lower limb edema). The surface electrocardiogram showed a sinus tachycardia at 101 cycles/min, an anterior hemiblock, and a left ventricular hypertrophy (Figure 1).
Figure 1. Regular sinus tachycardia with anterior hemiblock and left ventricular hypertrophy.
The frontal chest x-ray revealed global cardiomegaly with a supradiaphragmatic point, a double contour appearance of the right lower arch. At the level of the parenchyma, the presence of an encysted effusion on the right, a subpleural nodule above the fissure which itself is the site of a scissuritis were noted.
Biology had revealed a non-specific biological inflammatory syndrome with leukocytosis at 13100/mm3 with a predominance of polynuclear neutrophils, normochromic normocytic anemia at 9 g/dl and a positive CRP at 48 mg/l. Renal function was normal and hyponatremia was noted at 127.3 mEq/L on the blood ionogram, the kaliemia and chloremia were normal. Blood cultures were positive for streptococcus.
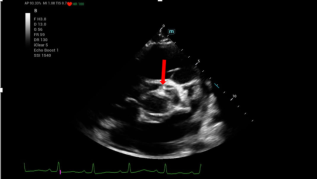
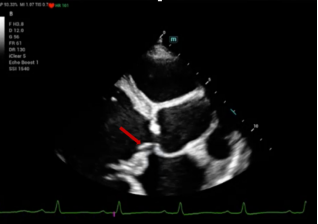
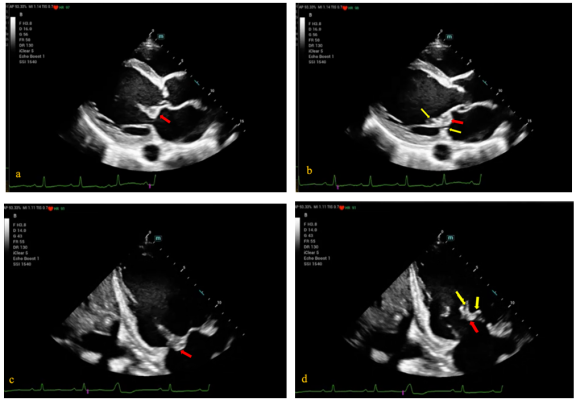
Transthoracic echocardiography showed bicuspid aortic type 1 LR (Figure 2). The aortic sigmoids were thickened, mutilated seats of vegetations hanging on the ventricular side (Figure 3) and responsible for an eccentric and severe leak (isthmic end-diastolic velocity of 75m/s) directed towards the mitral valve. On the mitral valve were noted the presence of vegetations on its ventricular side, at the level of the cords and on the atrial side (Figure 4). The atrial side was also the site of an aneurysmal sac with hyperechoic contents, probably thrombosed (Figure 4). On Doppler there was a severe mitral leak with a regurgitated volume of 122 ml/min and an orifice surface area of 0.86 cm2.
The diagnosis of mitro-aortic infectious endocarditis decompensating an aortic insufficiency on a bicuspid aortic valve with global heart failure was established, and the patient was started on diuretics and appropriate antibiotic therapy.
The evolution was complicated by the occurrence of a stroke and septic shock, leading to the patient's death after 34 days of hospitalization. No necropsy was done.
Figure 3. Transthoracic echocardiography in long axis parasternal section revealing thickened sigmoid bones with the visualization of vegetation (red arrow).
Figure 4. Transthoracic echocardiography in parasternal long axis section (a, b) and apical 2 cavities (c, d) showing the aneurysmal sac on the atrial side of the anterior leaflet of the mitral (red arrow) with thrombosed contents and the vegetations (yellow arrows) on the atrial and ventricular sides of the mitral.
3. Discussion
Aneurysm of the anterior mitral valve is a rare cardiac anomaly; its association with infective endocarditis of the aortic valve as in this patient is classic
[6]
Wang, Y., Wang, S., Chen, D. Mitral valve aneurysms: echocardiographic characteristics, formation mechanisms, and patient outcomes. Front Cardiovasc Med. 2023; 10: 1233926.
. Occasional cases of mitral aneurysm in patients without endocarditis, such as those with connective tissue diseases, pseudoxanthoma elasticum, Marfan syndrome, and myxomatous valve degeneration have been described
[5]
Guler, A., Karabay Can, Y., Gursoy Ozan, M. Clinical and echocardiographic evaluation of mitral valve aneurysms: a retrospective, single center study. Int J Cardiovasc Imaging. 2014; 30: 535-41.
The patient described in this report presented with a bicuspid aortic joint which in itself constitutes a vulnerability factor to infective endocarditis compared to the general population
[7]
Roberts, W. C. The congenitally bicuspid aortic valve. A study of 85 autopsy cases. Am J Cardiol. 1970; 26(1): 72-83.
. The occurrence of a mitral valve aneurysm in the bicuspid aorta without any endocarditis has also been described
[8]
Mohanty, V., Sharma, S. K., Deora, S. Rare association of aneurysm of anterior mitral leaflet with bicuspid aortic valve. Ann Afr Med. 2023; 22(4): 554-6.
The mechanism by which an aneurysm of the anterior mitral leaflet occurs in infective endocarditis remains poorly understood. Several hypotheses have been proposed, with the most widely accepted being that the infection induces inflammation and weakening of the valve tissue. This, combined with the mechanical forces exerted by the aortic regurgitation jet, leads to the formation of an aneurysmal sac on the mitral leaflet.
The clinical presentation is often that of structural heart disease generally associated with aortic insufficiency and/or mitral regurgitation. The diagnosis is made by transthoracic cardiac ultrasound, where the main diagnostic feature of mitral valve aneurysm remains the presence of a localized bulging structure of the mitral leaflet towards the left atrium, with systolic expansion and diastolic collapse. Transesophageal ultrasound and three-dimensional shows superiority due to the better characterization of the structures with better visualization of the atrial side of the mitral valve
[9]
Mollod, M., Felner, K. J., Felner, J. M. Mitral and tricuspid valve aneurysms evaluated by transesophageal echocardiography. Am J Cardiol. 1997; 79(9): 1269-72.
Kanzaki, Y, Yoshida, K, Hozumi, T. Evaluation of mitral valve lesions in patients with infective endocarditis by three-dimensional echocardiography]. J Cardiol. 1999; 33(1): 7-11.
[9, 10]
. The differential diagnoses that should be carefully considered, based on the ultrasound appearance, include mitral valve prolapse, mitral valve myxoma, a mitral valve cyst without endothelization, or a (congenital) mitral valve diverticulum. Careful two-dimensional analysis helps distinguish the aneurysm from other abnormalities
[11]
Triki, F., Kacem, A., Ellouze, M. Anévrysme de la valve mitrale antérieure: complication rare de l’endocardite infectieuse aortique. À propos d’un cas et revue de la littérature. Chirurgie Thoracique et Cardio-Vasculaire. 2015; 19(1): 57-9.
[11]
.
The cases of mitral valve aneurysm reported in the literature, particularly those described in a series of 13 cases by Vilacosta
[2]
Vilacosta, I., San Román, J. A., Sarriá, C. Clinical, anatomic, and echocardiographic characteristics of aneurysms of the mitral valve. Am J Cardiol. 1999; 84(1): 110-3.
, indicate that aneurysmal damage to the valves exclusively affects the mitral valve, primarily involving its anterior leaflet. However, there are a few rare cases where aneurysms have been observed in the posterior leaflet
[12]
Hara, L., El Hattab, F. Z., Radi, F. Z., Zarzur, J., Cherti, M. Perforated posterior mitral valve aneurysm: a rare complication of infective endocarditis: a case report. Pan Afr Med J. 2019; 32: 178.
The progression of the condition may lead to a rupture, which is a major concern due to its potential to cause significant mitral regurgitation. This can result in a swift and severe deterioration of hemodynamic status. Additionally, another possible complication involves embolism, where a thrombus that has formed within the aneurysmal sac, particularly after a rupture, can migrate and cause systemic embolic events. In reported patient, the aneurysmal sac was thrombotic, however, rupture could not be documented, although it could not be ruled out given the complications that occurred (notably a stroke) and the deterioration of the hemodynamic status. Despite significative advances in antibiotic therapy, intensive care, and surgical techniques, mitral valve aneurysm remains fatal as it was in the described case, highlighting the importance of early diagnosis and appropriate management, which is primarily surgical
[13]
Gajjar, T. P., Desai, N. B. True aneurysm of anterior mitral leaflet--a rare entity. J Thorac Cardiovasc Surg. 2012; 144(3): e93–5.
. The choice of therapeutic strategy, whether involving surgical intervention for the repairment or replacement of the mitral valve or a conservative management approach, will depend on the presence of ruptured or large aneurysms, severe hemodynamic disturbances, uncontrolled infections, or peripheral emboli
[6]
Wang, Y., Wang, S., Chen, D. Mitral valve aneurysms: echocardiographic characteristics, formation mechanisms, and patient outcomes. Front Cardiovasc Med. 2023; 10: 1233926.
. Despite the enthusiasm of some authors for medical management, it is now widely accepted that the cornerstone of treatment remains surgery
[12]
Hara, L., El Hattab, F. Z., Radi, F. Z., Zarzur, J., Cherti, M. Perforated posterior mitral valve aneurysm: a rare complication of infective endocarditis: a case report. Pan Afr Med J. 2019; 32: 178.
Anterior mitral valve aneurysm is a rare entity, usually a complication of aortic endocarditis. Its diagnosis is easy with echocardiography. Although the definitive treatment of MVA secondary to endocarditis is surgical, access to this procedure remains limited in sub-Saharan Africa due to insufficient technical resources.
Abbreviations
AVM
Anterior Mitral Valve Aneurysm
Author Contributions
Marguerite Téning Diouf: Collecting the case, acquiring echocardiography image, editing images, writing-review and editing
Papa Adama Faye: Writing original draft
Papa Momar Guissé: Acquiring echocardiography image
Rest of authors: Supervision
Funding
This work is not supported by any external funding.
Data Availability Statement
The data is available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
[1]
Tariq, M., Zahid, I., Sami, S. Rare aneurysm of anterior mitral valve leaflet-a case report. J Cardiothorac Surg. 2019; 14: 204.
Vilacosta, I., San Román, J. A., Sarriá, C. Clinical, anatomic, and echocardiographic characteristics of aneurysms of the mitral valve. Am J Cardiol. 1999; 84(1): 110-3.
Guler, A., Karabay Can, Y., Gursoy Ozan, M. Clinical and echocardiographic evaluation of mitral valve aneurysms: a retrospective, single center study. Int J Cardiovasc Imaging. 2014; 30: 535-41.
Mohanty, V., Sharma, S. K., Deora, S. Rare association of aneurysm of anterior mitral leaflet with bicuspid aortic valve. Ann Afr Med. 2023; 22(4): 554-6.
Mollod, M., Felner, K. J., Felner, J. M. Mitral and tricuspid valve aneurysms evaluated by transesophageal echocardiography. Am J Cardiol. 1997; 79(9): 1269-72.
Kanzaki, Y, Yoshida, K, Hozumi, T. Evaluation of mitral valve lesions in patients with infective endocarditis by three-dimensional echocardiography]. J Cardiol. 1999; 33(1): 7-11.
[11]
Triki, F., Kacem, A., Ellouze, M. Anévrysme de la valve mitrale antérieure: complication rare de l’endocardite infectieuse aortique. À propos d’un cas et revue de la littérature. Chirurgie Thoracique et Cardio-Vasculaire. 2015; 19(1): 57-9.
[12]
Hara, L., El Hattab, F. Z., Radi, F. Z., Zarzur, J., Cherti, M. Perforated posterior mitral valve aneurysm: a rare complication of infective endocarditis: a case report. Pan Afr Med J. 2019; 32: 178.
Diouf, M. T., Faye, P. A., Guissé, P. M., Mingou, J. S., Kane, A. (2024). Aneurysm of the Anterior Mitral Valve Complicating Infectious Mitro-Aortic Endocarditis in a Biscuspid Aortic Valve: About a Case. Cardiology and Cardiovascular Research, 8(3), 87-91. https://doi.org/10.11648/j.ccr.20240803.12
Diouf, M. T.; Faye, P. A.; Guissé, P. M.; Mingou, J. S.; Kane, A. Aneurysm of the Anterior Mitral Valve Complicating Infectious Mitro-Aortic Endocarditis in a Biscuspid Aortic Valve: About a Case. Cardiol. Cardiovasc. Res.2024, 8(3), 87-91. doi: 10.11648/j.ccr.20240803.12
Diouf MT, Faye PA, Guissé PM, Mingou JS, Kane A. Aneurysm of the Anterior Mitral Valve Complicating Infectious Mitro-Aortic Endocarditis in a Biscuspid Aortic Valve: About a Case. Cardiol Cardiovasc Res. 2024;8(3):87-91. doi: 10.11648/j.ccr.20240803.12
@article{10.11648/j.ccr.20240803.12,
author = {Marguerite Téning Diouf and Papa Adama Faye and Papa Momar Guissé and Joseph Salvator Mingou and Abdoul Kane},
title = {Aneurysm of the Anterior Mitral Valve Complicating Infectious Mitro-Aortic Endocarditis in a Biscuspid Aortic Valve: About a Case
},
journal = {Cardiology and Cardiovascular Research},
volume = {8},
number = {3},
pages = {87-91},
doi = {10.11648/j.ccr.20240803.12},
url = {https://doi.org/10.11648/j.ccr.20240803.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ccr.20240803.12},
abstract = {Mitral valve aneurysm is a rare condition usually associated with aortic valve endocarditis. The mechanism, poorly understood, generally includes a regurgitant infectious flow originating from the aortic valve, direct contact with vegetation and direct propagation, through adjacent structures, such as the mitro-aortic intervalvular fibrous body. This report details the case of a 56-year-old patient followed for severe bicuspid aortic insufficiency of the aortic valve for 4 months and admitted to heart failure due to infectious endocarditis with a fatal outcome. Physical examination revealed aortic and mitral insufficiency syndrome and congestive heart failure. Transthoracic echocardiography revealed type 1 L-R bicuspid heart disease and leaking polyvalvulopathy with severe eccentric aortic and severe mitral regurgitation. The aortic and mitral valves were the seat of the vegetations. The mitral valve was the seat on its atrial side of a contained aneurysmal sac with thrombosed hyperechogenicity. Blood cultures were positive for streptococci and probabilistic dual antibiotic therapy was started. The patient was unable to benefit from surgical treatment. However, the patient died following complications such as ischemic stroke and septic shock. A necropsy was not done.
},
year = {2024}
}
TY - JOUR
T1 - Aneurysm of the Anterior Mitral Valve Complicating Infectious Mitro-Aortic Endocarditis in a Biscuspid Aortic Valve: About a Case
AU - Marguerite Téning Diouf
AU - Papa Adama Faye
AU - Papa Momar Guissé
AU - Joseph Salvator Mingou
AU - Abdoul Kane
Y1 - 2024/08/30
PY - 2024
N1 - https://doi.org/10.11648/j.ccr.20240803.12
DO - 10.11648/j.ccr.20240803.12
T2 - Cardiology and Cardiovascular Research
JF - Cardiology and Cardiovascular Research
JO - Cardiology and Cardiovascular Research
SP - 87
EP - 91
PB - Science Publishing Group
SN - 2578-8914
UR - https://doi.org/10.11648/j.ccr.20240803.12
AB - Mitral valve aneurysm is a rare condition usually associated with aortic valve endocarditis. The mechanism, poorly understood, generally includes a regurgitant infectious flow originating from the aortic valve, direct contact with vegetation and direct propagation, through adjacent structures, such as the mitro-aortic intervalvular fibrous body. This report details the case of a 56-year-old patient followed for severe bicuspid aortic insufficiency of the aortic valve for 4 months and admitted to heart failure due to infectious endocarditis with a fatal outcome. Physical examination revealed aortic and mitral insufficiency syndrome and congestive heart failure. Transthoracic echocardiography revealed type 1 L-R bicuspid heart disease and leaking polyvalvulopathy with severe eccentric aortic and severe mitral regurgitation. The aortic and mitral valves were the seat of the vegetations. The mitral valve was the seat on its atrial side of a contained aneurysmal sac with thrombosed hyperechogenicity. Blood cultures were positive for streptococci and probabilistic dual antibiotic therapy was started. The patient was unable to benefit from surgical treatment. However, the patient died following complications such as ischemic stroke and septic shock. A necropsy was not done.
VL - 8
IS - 3
ER -
Biography:
Joseph Salvator Mingou: Cardiology department at Dalal Jamm Hospital, Senior Lecturer at the University Cheikh Anta DIOP of Dakar, cardiologist specialized interventional cardiologist.
Biography:
Abdoul Kane: full professor at Cheikh Anta DIOP University of Dakar, Head of the Cardiology Department at Dalal Jamm Hospital, Chair of Cardiology.
Diouf, M. T., Faye, P. A., Guissé, P. M., Mingou, J. S., Kane, A. (2024). Aneurysm of the Anterior Mitral Valve Complicating Infectious Mitro-Aortic Endocarditis in a Biscuspid Aortic Valve: About a Case. Cardiology and Cardiovascular Research, 8(3), 87-91. https://doi.org/10.11648/j.ccr.20240803.12
Diouf, M. T.; Faye, P. A.; Guissé, P. M.; Mingou, J. S.; Kane, A. Aneurysm of the Anterior Mitral Valve Complicating Infectious Mitro-Aortic Endocarditis in a Biscuspid Aortic Valve: About a Case. Cardiol. Cardiovasc. Res.2024, 8(3), 87-91. doi: 10.11648/j.ccr.20240803.12
Diouf MT, Faye PA, Guissé PM, Mingou JS, Kane A. Aneurysm of the Anterior Mitral Valve Complicating Infectious Mitro-Aortic Endocarditis in a Biscuspid Aortic Valve: About a Case. Cardiol Cardiovasc Res. 2024;8(3):87-91. doi: 10.11648/j.ccr.20240803.12
@article{10.11648/j.ccr.20240803.12,
author = {Marguerite Téning Diouf and Papa Adama Faye and Papa Momar Guissé and Joseph Salvator Mingou and Abdoul Kane},
title = {Aneurysm of the Anterior Mitral Valve Complicating Infectious Mitro-Aortic Endocarditis in a Biscuspid Aortic Valve: About a Case
},
journal = {Cardiology and Cardiovascular Research},
volume = {8},
number = {3},
pages = {87-91},
doi = {10.11648/j.ccr.20240803.12},
url = {https://doi.org/10.11648/j.ccr.20240803.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ccr.20240803.12},
abstract = {Mitral valve aneurysm is a rare condition usually associated with aortic valve endocarditis. The mechanism, poorly understood, generally includes a regurgitant infectious flow originating from the aortic valve, direct contact with vegetation and direct propagation, through adjacent structures, such as the mitro-aortic intervalvular fibrous body. This report details the case of a 56-year-old patient followed for severe bicuspid aortic insufficiency of the aortic valve for 4 months and admitted to heart failure due to infectious endocarditis with a fatal outcome. Physical examination revealed aortic and mitral insufficiency syndrome and congestive heart failure. Transthoracic echocardiography revealed type 1 L-R bicuspid heart disease and leaking polyvalvulopathy with severe eccentric aortic and severe mitral regurgitation. The aortic and mitral valves were the seat of the vegetations. The mitral valve was the seat on its atrial side of a contained aneurysmal sac with thrombosed hyperechogenicity. Blood cultures were positive for streptococci and probabilistic dual antibiotic therapy was started. The patient was unable to benefit from surgical treatment. However, the patient died following complications such as ischemic stroke and septic shock. A necropsy was not done.
},
year = {2024}
}
TY - JOUR
T1 - Aneurysm of the Anterior Mitral Valve Complicating Infectious Mitro-Aortic Endocarditis in a Biscuspid Aortic Valve: About a Case
AU - Marguerite Téning Diouf
AU - Papa Adama Faye
AU - Papa Momar Guissé
AU - Joseph Salvator Mingou
AU - Abdoul Kane
Y1 - 2024/08/30
PY - 2024
N1 - https://doi.org/10.11648/j.ccr.20240803.12
DO - 10.11648/j.ccr.20240803.12
T2 - Cardiology and Cardiovascular Research
JF - Cardiology and Cardiovascular Research
JO - Cardiology and Cardiovascular Research
SP - 87
EP - 91
PB - Science Publishing Group
SN - 2578-8914
UR - https://doi.org/10.11648/j.ccr.20240803.12
AB - Mitral valve aneurysm is a rare condition usually associated with aortic valve endocarditis. The mechanism, poorly understood, generally includes a regurgitant infectious flow originating from the aortic valve, direct contact with vegetation and direct propagation, through adjacent structures, such as the mitro-aortic intervalvular fibrous body. This report details the case of a 56-year-old patient followed for severe bicuspid aortic insufficiency of the aortic valve for 4 months and admitted to heart failure due to infectious endocarditis with a fatal outcome. Physical examination revealed aortic and mitral insufficiency syndrome and congestive heart failure. Transthoracic echocardiography revealed type 1 L-R bicuspid heart disease and leaking polyvalvulopathy with severe eccentric aortic and severe mitral regurgitation. The aortic and mitral valves were the seat of the vegetations. The mitral valve was the seat on its atrial side of a contained aneurysmal sac with thrombosed hyperechogenicity. Blood cultures were positive for streptococci and probabilistic dual antibiotic therapy was started. The patient was unable to benefit from surgical treatment. However, the patient died following complications such as ischemic stroke and septic shock. A necropsy was not done.
VL - 8
IS - 3
ER -