Background: Post-surgical motor deficits are a frequent complication in neuro-oncologic patients and can significantly affect functional recovery. Transcranial magnetic stimulation (TMS) has emerged as a potential therapeutic modality to facilitate motor rehabilitation. This systematic review examined the effectiveness and safety of TMS in promoting motor recovery following brain tumor surgery. Methods: A systematic review of four studies evaluating TMS for postoperative motor rehabilitation in patients with brain tumors was performed. Outcome measures included motor function assessments using the British Medical Research Council (BMRC) scale, Fugl-Meyer Assessment (FMA), and Karnofsky Performance Status (KPS), as well as the incidence of adverse events. Results: The effects of TMS on motor recovery were inconsistent across studies, with some demonstrating improvements in BMRC and FMA scores, while others reported limited therapeutic benefit. Overall, TMS was generally well tolerated, with only minimal adverse events documented. Conclusions: TMS may represent a safe and promising adjunctive intervention for postoperative motor recovery in brain tumor patients; however, the current evidence remains insufficient to establish definitive clinical benefit. Further large-scale prospective studies using standardized treatment protocols are necessary to clarify its therapeutic efficacy and long-term safety profile.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Transcranial Magnetic Stimulation, Brain Tumors, Motor Recovery, Neuromodulation
1. Background
Transcranial magnetic stimulation is a non-invasive neuromodulation modality with a favorable safety profile that can be administered without the need for general anesthesia or sedation. It operates by passing rapidly alternating electrical currents through a coil, producing magnetic fields that penetrate the scalp and skull painlessly to stimulate targeted cortical regions. This stimulation alters neuronal excitability and facilitates neuroplastic changes, thereby promoting functional reorganization of disrupted neural networks
. Three types of general TMS protocols exist, including single-pulse, paired pulse, and repetitive TMS (rTMS). In particular, rTMS is used to facilitate excitation or inhibition of cortical areas and is often used in clinical practice. In rTMS, multiple single-pulse stimuli are delivered at a specified time duration, frequency, and intensity with effects varying according to stimulation parameters usually at 1-20Hz
[3]
Maeda F, Keenan JP, Tormos JM, Topka H, Pascual-Leone A. Modulation of corticospinal excitability by repetitive transcranial magnetic stimulation. Clin Neurophysiol. 2000; 111(5): 800-5.
TMS is already established in treating depression and addressing stroke rehabilitation but there is an increasing number of indications for its use. Recently, studies on its effect in improving the quality of sleep, improving chemo-induced cognitive impairment and Alzheimer’s disease are being published
[4]
Kuo PH, Chen AYC, Rodriguez RJ, Stuehm C, Chalasani P, Chen NK, Chou YH. (2023) Transcranial Magnetic Stimulation for the Treatment of Chemo Brain. Sensors. 23, 8017.
. Though the specific treatment parameters and exact mechanism are not yet well established, TMS is also becoming a promising treatment in neuro-oncologic patients especially now that the myth on its increased seizure risk has been debunked as long as the recommended regimen is given
[5]
Rossi S, Antal A, Bestmann S, et al. (2021) Safety and recommendations for TMS use in healthy subjects and patient populations, with updates on training, ethical and regulatory issues: Expert Guidelines. Clin Neurophysiol. Jan; 132(1): 269-306.
Hu Y, Zhu Y, Wen X, Zeng F, Feng Y, Xu Z, Xu F, Wang J. (2022). Repetitive transcranial magnetic stimulation regulates neuroinflammation, relieves hyperalgesia and reverses despair-like behaviour in chronic constriction injury rats. European Journal of Neuroscience, 56(6), 4930–4947.
The treatment of patients with brain tumor usually involves surgical intervention. With the complexity of the brain and the multitude of symptomatic presentations of neuro-oncologic patients, the risk of neurological damage is a concern, with emphasis on lesions located in areas near typically motor regions, such as primary motor areas or even subcortical structures in contact with the corticospinal tract, due to the possibility of partial or structural damage to the motor pathway
[7]
Krivosheya D, Prabhu SS, Weinberg JS, Sawaya R. (2016) Technical principles in glioma surgery and preoperative considerations. J Neurooncol. 130(2): 243–252.
. In the Glioma Outcomes Project in the United States, a database of 800 patients who had undergone brain surgery for the excision of tumor, showed that approximately 32% of patients reported motor deficits
[8]
Chang SM et al. (2003) Perioperative complications and neurological outcomes of first and second craniotomies among patients enrolled in the Glioma Outcome Project. J Neurosurg 98(6): 1175–1181.
. Given the high risk for motor complication and the evidence for using TMS for neurorehabilitation for other neurologic diseases like stroke, there is reason to believe that TMS could be beneficial post-operatively for recovery in patients with brain tumors. In a case report by Kakuda et al., a patient with a left subfrontal glioma who underwent surgery with residual right upper extremity hemiparesis was already stable at five years after surgery. She was already considered to have reached a probable plateau state of motor functional recovery of the affected upper limb in spite of conventional occupational therapy. However, low frequency 1Hz rTMS was used with each session consisting of 1200 pulses for 22 daily sessions and experienced immediate improvement in right upper extremity function with further improvement upon follow up four weeks the rTMS treatment
[9]
Kakuda W, Abo M, Kobayashi K, Momosaki R, Yokoi A, Ito H, Umemori T. (2010) Low-frequency rTMS combined with intensive occupational therapy for upper limb hemiparesis after brain tumour resection. Brain Inj. 24(12): 1505-10.
. Because of this, several studies are now looking at TMS as treatment for post-surgical motor dysfunction.
2. Objectives
This study aimed to identify available literature and to perform a systematic review of all available data on the use of transcranial magnetic stimulation in the post-surgical motor recovery in brain tumor patients.
3. Methodology
This is a systematic review of randomized controlled trials and prospective cohorts. Systematic scoping review was done following the Preferred Reporting Items for Systematic Reviews (PRISMA) recommendations
[10]
Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. 2009; 6: e1–e34.
. The article was not registered in any systematic review protocol database.
3.1. Inclusion and Exclusion Criteria
Studies eligible for inclusion were studies presenting confirmed diagnosis of brain tumor (primary or metastatic), patients >18 y/o, using TMS for post-surgical motor rehabilitation. Also, articles published in peer- reviewed journals, and written only in English were included. Articles that could not be retrieved as full articles through institutional database access or by asking the involved authors were excluded.
3.2. Search Strategy
All authors searched the PubMed, Embase, Cochrane Library, Web of Science and Clinicaltrials.gov databases from inception through December 2025. The literature search strategy was developed using Medical Subject Headings (MeSH) and relevant keyword combinations, including terms related to “transcranial magnetic stimulation”, “brain tumors”, “malignancy”, “cancer”, “postsurgical recovery”, “motor deficits”, and “hemiparesis”. These terms were systematically combined using the Boolean operators “OR” and “AND” to broaden or refine the search by linking related and distinct concepts. Study selection was performed in two stages: an initial screening of titles, abstracts, and keywords, followed by full-text evaluation of potentially eligible articles.
3.3. Data Extraction
Data from each eligible study were extracted by one author (R. De Roxas) and confirmed by another author (M. dela Vega). The required information included the author’s name, publication year, number of patients, TMS regimen received, efficacy in the improvement of post-surgical motor strength and adverse effects.
3.4. Risk of Bias Assessment
The methodological rigor of the included studies was independently evaluated by two reviewers (R. De Roxas and A. Cabungcal) using the revised Cochrane Risk of Bias Tool 2 (RoB 2)
. This structured instrument assesses potential sources of bias across key methodological domains, including study design, randomization procedures, and blinding. Based on these domain-level assessments, an overall risk-of-bias judgment was assigned through the RoB 2 algorithm and categorized as low risk, some concerns, or high risk of bias (Table 1).
4. Results
4.1. Study Identification and Selection
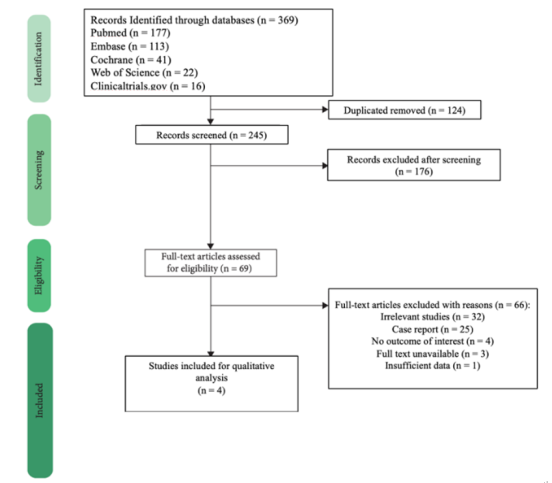
A total of 369 studies were identified from the PubMed (n=177), EMBASE (n=113), Cochrane Library (n=41), Web of Science (n=22) and clinicaltrials.gov (n=16) databases. After removing duplicates, the remaining studies were screened for eligibility. A total of 124 records were excluded due to duplicate titles and another 176 records were removed as determined by screening titles and abstracts. Therefore, 69 studies were assessed with a full-text review. Sixty-five studies were excluded as they were deemed irrelevant, had no full-text available or had inadequate data relevant to the outcomes of interest. Finally, four studies involving 199 patients were included. The detailed PRISMA flow diagram is presented in Figure 1.
The characteristics and outcomes of interest at baseline of the three included studies are listed. Three of the studies were double-blind, parallel, sham-controlled RCTs while the 4th study is a prospective cohort. The included studies enrolled a total of 199 patients diagnosed with brain tumor who had a motor deficit after surgery and eventually underwent TMS.
Table 1. Risk of Bias Assessment.
RISK Domain
Random sequence generation
Allocation concealment
Blinding of participants and personnel
Deviations from intended interventions
Missing outcome data
Measurement of the outcome
Rosenstock et al./2024
UNCLEAR
UNCLEAR
LOW
LOW
UNCLEAR
LOW
Engelhardt et al., 2024
LOW
LOW
LOW
UNCLEAR
LOW
LOW
Ille et al., 2021
LOW
LOW
LOW
LOW
LOW
LOW
Tang et al./2022
HIGH
HIGH
HIGH
UNCLEAR
LOW
LOW
Table 2. Study Characteristics.
Author, Year
Study Type
Number of patients
TMS regimen received
Efficacy measure on motor strength
Adverse events
Rosenstock et al. (2025)
Multicentric randomized controlled trial
135
Low-frequency rTMS treatment to the contralateral hemisphere according to center-specific protocols for 7–10 days
Functional motor status was assessed using BMRC score, FMA and KPS score
Accelerated Theta burst stimulation sessions were administered per day for a maximum period of 2 weeks with an hour gap between sessions
Lower extremity functional scales (LEFS) and upper extremity functional scales (UEFS) were administered either together or individually
No patients reported any seizures following rTMS treatment. The adverse events noted are fatigue, headache and scalp discomfort.
In the study of Rosenstock et al., patients in the treatment group had a higher probability of a better postoperative BMRC score immediately after treatment (3.28, 95%CI: 1.08–9.99) and after 3 months (2.03, 95%CI: 0.65 to 6.39) compared to the sham group. This finding is also the same with the improvement in the KPS score where patients in the treatment group had a substantially higher postoperative KPS score immediately after treatment (11, 95% CI: 2-19) and after 3 months (11, 95% CI: 2–20) compared to patients in the sham group. However, patients in the treatment group had a similar postoperative FMA score immediately after treatment (0.28, 95% CI: -0.34–0.90) and after 3 months (0.14, 95% CI: -0.52 to 0.81) compared to patients in the sham group
[12]
Rosenstock T, Picht T, Engelhardt M, Grittner U, Mönch M, Vajkoczy P, Lavrador JP, Mirallave-Pescador A, Vergani F, Schwendner M, Schroeder A, Kram L, Zhang H, Prabhu S, Prinsloo S, Meyer B, Ille S, Krieg SM. (2025) Improving postsurgical paresis in brain tumor patients by transcranial magnetic stimulation. J Neurooncol. 172(2): 417-428.
In the study by Engelhardt et al., patients in the rTMS group presented with slightly better Fugl Meyer Scores compared to the control group (5.1, 95% CI-16.0-26.1; p=0.631) three months postoperatively although the difference is not significant. Additionally, the BMRC score for distal upper extremity muscles was better at month 1 (23.20, 95%CI 1.02-527.30; p=0.049) compared to the sham group. As for the adverse events, all patients tolerated the intervention well and completed stimulation at the designed intensity. The most common adverse events were headaches, followed my mild nausea and dizziness
[13]
Engelhardt M, Schneider H, Reuther J, Grittner U, Vajkoczy P, Picht T and Rosenstock T (2024) Low-frequency repetitive transcranial magnetic stimulation in patients with motor deficits after brain tumor resection: a randomized, double-blind, sham-controlled trial. Front. Oncol. 14: 1368924.
In the study by Ille et al., the change in FMA score on follow-up was statistically significant showing mean improvement from 31.93 (95%CI 22.6-41.25) points in the rTMS group while it was 4.2 (95%CI -4.14-12.54) points in the sham group. No change in the KPS score was noted
[14]
Ille S, Kelm A, Schroeder A, Albers LE, Negwer C, Butenschoen VM, Sollmann N, Picht T, Vajkoczy P, Meyer B, Krieg SM. (2021) Navigated repetitive transcranial magnetic stimulation improves the outcome of postsurgical paresis in glioma patients - A randomized, double-blinded trial. Brain Stimul. 14(4): 780-787.
In the study by Tang et al., seven out of the nine patients who were administered the LEFS showed at least a 9-point improvement between post- treatment and baseline. On the other hand, eight out of the eight patients who were administered the UEFS also had at least a 9-point improvement between post- treatment and baseline. Reported adverse events of TMS were fatigue (58.3%), headache (25%) scalp discomfort at the stimulation site (33.3%), and facial twitching due to stimulation (8.3%)
[15]
Tang SJ, Holle J, Lesslar O, Teo C, Sughrue M, Yeung J. (2022) Improving quality of life post-tumor craniotomy using personalized, parcel-guided TMS: safety and proof of concept. J Neurooncol. 160(2): 413-422.
Overall, the data demonstrate a variable degree of improvement in the post-surgical motor strength function across different scores. Both studies by Rosenstock et al. and Engelhardt et al. showed improvement in BMRC scores but fail to show significant improvement in the FMA scores. The study of Ille et al. interestingly showed a significant improvement in the FMA scores. The BMRC score is a widely used grading system that assessed contractile muscle strength on a scale from 0 – 5 with high scores indicating greater strength
[16]
Riddoch BG. (1943) Aids to the Investigation of Peripheral Nerve Injuries. Journal of the American Medical Association. 122(4): 266.
. On the other hand, the FMA score is a more detailed scoring system designed to evaluate motor functioning, sensation, balance and joint range of motion with a maximum score of 100 points
[17]
Fugl-Meyer AR, Jääskö L, Leyman I, Olsson S, Steglind S. (1975) The post-stroke hemiplegic patient. 1. a method for evaluation of physical performance. Scand J Rehabil Med. 7: 13–31.
. The study of Tang et al. uses LEFS and UEFS which are questionnaires containing 20 questions about the patient’s ability to perform everyday tasks in the lower and upper extremities respectively
[18]
Binkley JM, Stratford PW, Lott SA, Riddle DL. (1999) The lower extremity functional scale (LEFS): scale development, measurement properties, and clinical application. Phys Ther. 79: 371-383.
. The lack of a standardized scale to measure the improvement of motor strength after TMS makes it difficult to really make a more generalizable conclusion. Moreso, a specific neuro-oncologic tool to assess patients might be helpful. Although the study by Rosenstock et al. and Ille et al. used the KPS score, which is a widely used tool to measure the functional performance of cancer patients, it is not really a direct measure of motor function
[19]
Mor V Lalıberte L Morrıs JN Wıemann M. (2006) The Karnofsky performance status scale an examination of its reliability and validity in a research setting. Cancer. 1: 2002.
Heterogeneity in study populations across studies also likely contributed to variability in results. Only the study by Ille et al. showed significant improvement in FMA scores in the rTMS group compared to the sham group. The study has more rigorous inclusion criteria, enrolling only patients with documented subcortical ischemia on post-operative imaging and preserved motor evoked potentials (MEPs). A drop or loss of MEPs during intraoperative monitoring in brain tumor surgery is a neurophysiological marker of a permanent motor deficit
[20]
Giampiccolo D, Parisi C, Meneghelli P, Tramontano V, Basaldella F, Pasetto M, Pinna G, Cattaneo L, Sala F. (2021) Long-term motor deficit in brain tumour surgery with preserved intra-operative motor-evoked potentials. Brain Commun. Jan 23; 3(1): fcaa226.
. Conversely, preserved MEPs is indicative of less severe injury and can be predictive of a potential for motor recovery. In the subgroup analyses done in the studies by Rosenstock et al. and Engelhardt et al., treatment effects are more pronounced in patients with weakness due to subcortical ischemia rather than direct injury to the motor cortex. This is similar to what is observed in stroke patients with subcortical infarcts treated with rTMS
[21]
Hsu WY, Cheng CH, Liao KK, Lee IH, Lin YY. (2012) Effects of repetitive transcranial magnetic stimulation on motor functions in patients with stroke: a meta-analysis. Stroke. 2012 Jul; 43(7): 1849-57.
Hildesheim FE, Silver AN, Dominguez-Vargas A-U, Andrushko JW, Edwards JD, Dancause N and Thiel A. (2022) Predicting Individual Treatment Response to rTMS for Motor Recovery After Stroke: A Review and the CanStim Perspective. Front. Rehabilit. Sci. 3: 795335.
, indicating that rTMS can better induce neuroplasticity and motor recovery in this subgroup of patients.
Both the studies of Engelhardt et al. and Ille et al. used TMS protocol with a stimulation of 1 Hz for 15 min (900 pulses) at an intensity of 110% resting motor threshold applied to the contralateral hemisphere handled perpendicular to the gyrus of the brain. However, in the studies of Rosenstock et al. and Ille et al., there are a number of TMS protocol used based on the institutional practice. The lack of a standard protocol, specifically for brain tumor patients, makes it also difficult to make a conclusion based on this review.
As to the safety of TMS, all the studies included reported no serious adverse events in the duration of the study. Headache, nausea, dizziness, fatigue and scalp discomfort were the adverse events reported. The lack of seizures after TMS use in the 199 brain tumor patients included in this review is further reassuring that it can be used safely in neuro-oncologic patients, given that these patients are seen to be at higher risk for seizures. However, the overall risk must be evaluated on a case-by-case basis.
6. Conclusion
TMS might be a promising tolerable therapy for acute post-surgical paresis after brain tumor resection to improve motor recovery, especially in a select cases related to subcortical ischemia. However, it should be noted that more research is needed to adequately account for confounding variables and the standardization of TMS protocol administered to patients. Once this is achieved, a facilitation of motor recovery using TMS could potentially reduce the disease burden in patients, leading to a better tolerability of adjuvant treatments, faster return to work and higher quality of life.
7. Limitations
The findings of this systematic review should be interpreted in light of several limitations. First, the available evidence is characterized by substantial heterogeneity across studies, including differences in patient populations, stimulation targets, TMS protocols used, outcome measures, and follow-up periods. This variability limits the comparability of studies and reduces the ability to draw definitive conclusions regarding efficacy and safety. Second, although numerous therapeutic protocols have been explored and varying degrees of clinical success have been reported, the current evidence base remains largely constrained by methodological inconsistencies. These factors may contribute to variability in treatment response and limit the generalizability of findings and scores received by the patients. Lastly, the mechanisms underlying differential responsiveness to TMS in brain tumor patients remain insufficiently understood. Accordingly, larger prospective studies with robust methodological design, standardized protocols, and well-defined outcome measures are warranted to better delineate the therapeutic efficacy of TMS and to identify reliable predictors of motor strength recovery.
Abbreviations
BMRC
British Medical Research Council
CI.
Confident Interval
FMA
Fugl-Meyer Assessment
KPS
Karnofsky Performance Status
LEFS
Lower Extremity Functional Scales
MeSH.
Medical Subject Headings
PRISMA
Preferred Reporting Items for Systematic Reviews
RCT.
Randomized Controlled Trial
RoB
2 Risk of Bias Tool 2
rTMS
Repetitive Transcranial Magnetic Stimulation
TMS
Transcranial Magnetic Stimulation
UEFS
Upper Extremity Functional Scales
Author Contributions
Ranhel De Roxas: Conceptualization, Data curation, Writing – original draft
Ana Gabriela Cabungcal: Data curation, Formal analysis, Methodology
Mia Patrice Dela Vega: Resources, Data curation, Methodology, Validation, Writing – review & editing
Marian Sheryl Milo: Resources, Formal analysis, Data curation
Rossi S, Antal A, Bestmann S, et al. (2021) Safety and recommendations for TMS use in healthy subjects and patient populations, with updates on training, ethical and regulatory issues: Expert Guidelines. Clin Neurophysiol. Jan; 132(1): 269-306.
Hu Y, Zhu Y, Wen X, Zeng F, Feng Y, Xu Z, Xu F, Wang J. (2022). Repetitive transcranial magnetic stimulation regulates neuroinflammation, relieves hyperalgesia and reverses despair-like behaviour in chronic constriction injury rats. European Journal of Neuroscience, 56(6), 4930–4947.
Chang SM et al. (2003) Perioperative complications and neurological outcomes of first and second craniotomies among patients enrolled in the Glioma Outcome Project. J Neurosurg 98(6): 1175–1181.
Kakuda W, Abo M, Kobayashi K, Momosaki R, Yokoi A, Ito H, Umemori T. (2010) Low-frequency rTMS combined with intensive occupational therapy for upper limb hemiparesis after brain tumour resection. Brain Inj. 24(12): 1505-10.
Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. 2009; 6: e1–e34.
Rosenstock T, Picht T, Engelhardt M, Grittner U, Mönch M, Vajkoczy P, Lavrador JP, Mirallave-Pescador A, Vergani F, Schwendner M, Schroeder A, Kram L, Zhang H, Prabhu S, Prinsloo S, Meyer B, Ille S, Krieg SM. (2025) Improving postsurgical paresis in brain tumor patients by transcranial magnetic stimulation. J Neurooncol. 172(2): 417-428.
Engelhardt M, Schneider H, Reuther J, Grittner U, Vajkoczy P, Picht T and Rosenstock T (2024) Low-frequency repetitive transcranial magnetic stimulation in patients with motor deficits after brain tumor resection: a randomized, double-blind, sham-controlled trial. Front. Oncol. 14: 1368924.
Ille S, Kelm A, Schroeder A, Albers LE, Negwer C, Butenschoen VM, Sollmann N, Picht T, Vajkoczy P, Meyer B, Krieg SM. (2021) Navigated repetitive transcranial magnetic stimulation improves the outcome of postsurgical paresis in glioma patients - A randomized, double-blinded trial. Brain Stimul. 14(4): 780-787.
Tang SJ, Holle J, Lesslar O, Teo C, Sughrue M, Yeung J. (2022) Improving quality of life post-tumor craniotomy using personalized, parcel-guided TMS: safety and proof of concept. J Neurooncol. 160(2): 413-422.
Fugl-Meyer AR, Jääskö L, Leyman I, Olsson S, Steglind S. (1975) The post-stroke hemiplegic patient. 1. a method for evaluation of physical performance. Scand J Rehabil Med. 7: 13–31.
Mor V Lalıberte L Morrıs JN Wıemann M. (2006) The Karnofsky performance status scale an examination of its reliability and validity in a research setting. Cancer. 1: 2002.
Giampiccolo D, Parisi C, Meneghelli P, Tramontano V, Basaldella F, Pasetto M, Pinna G, Cattaneo L, Sala F. (2021) Long-term motor deficit in brain tumour surgery with preserved intra-operative motor-evoked potentials. Brain Commun. Jan 23; 3(1): fcaa226.
Hsu WY, Cheng CH, Liao KK, Lee IH, Lin YY. (2012) Effects of repetitive transcranial magnetic stimulation on motor functions in patients with stroke: a meta-analysis. Stroke. 2012 Jul; 43(7): 1849-57.
Hildesheim FE, Silver AN, Dominguez-Vargas A-U, Andrushko JW, Edwards JD, Dancause N and Thiel A. (2022) Predicting Individual Treatment Response to rTMS for Motor Recovery After Stroke: A Review and the CanStim Perspective. Front. Rehabilit. Sci. 3: 795335.
Roxas, R. D., Cabungcal, A. G., Vega, M. P. D., Milo, M. S. (2026). Efficacy and Safety of Transcranial Magnetic Stimulation for Post-surgical Motor Strength Recovery in
Neuro-oncologic Patients: A Systematic Review. Clinical Medicine Research, 15(3), 34-40. https://doi.org/10.11648/j.cmr.20261503.11
Roxas, R. D.; Cabungcal, A. G.; Vega, M. P. D.; Milo, M. S. Efficacy and Safety of Transcranial Magnetic Stimulation for Post-surgical Motor Strength Recovery in
Neuro-oncologic Patients: A Systematic Review. Clin. Med. Res.2026, 15(3), 34-40. doi: 10.11648/j.cmr.20261503.11
Roxas RD, Cabungcal AG, Vega MPD, Milo MS. Efficacy and Safety of Transcranial Magnetic Stimulation for Post-surgical Motor Strength Recovery in
Neuro-oncologic Patients: A Systematic Review. Clin Med Res. 2026;15(3):34-40. doi: 10.11648/j.cmr.20261503.11
@article{10.11648/j.cmr.20261503.11,
author = {Ranhel De Roxas and Ana Gabriela Cabungcal and Mia Patrice Dela Vega and Marian Sheryl Milo},
title = {Efficacy and Safety of Transcranial Magnetic Stimulation for Post-surgical Motor Strength Recovery in
Neuro-oncologic Patients: A Systematic Review},
journal = {Clinical Medicine Research},
volume = {15},
number = {3},
pages = {34-40},
doi = {10.11648/j.cmr.20261503.11},
url = {https://doi.org/10.11648/j.cmr.20261503.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.cmr.20261503.11},
abstract = {Background: Post-surgical motor deficits are a frequent complication in neuro-oncologic patients and can significantly affect functional recovery. Transcranial magnetic stimulation (TMS) has emerged as a potential therapeutic modality to facilitate motor rehabilitation. This systematic review examined the effectiveness and safety of TMS in promoting motor recovery following brain tumor surgery. Methods: A systematic review of four studies evaluating TMS for postoperative motor rehabilitation in patients with brain tumors was performed. Outcome measures included motor function assessments using the British Medical Research Council (BMRC) scale, Fugl-Meyer Assessment (FMA), and Karnofsky Performance Status (KPS), as well as the incidence of adverse events. Results: The effects of TMS on motor recovery were inconsistent across studies, with some demonstrating improvements in BMRC and FMA scores, while others reported limited therapeutic benefit. Overall, TMS was generally well tolerated, with only minimal adverse events documented. Conclusions: TMS may represent a safe and promising adjunctive intervention for postoperative motor recovery in brain tumor patients; however, the current evidence remains insufficient to establish definitive clinical benefit. Further large-scale prospective studies using standardized treatment protocols are necessary to clarify its therapeutic efficacy and long-term safety profile.},
year = {2026}
}
TY - JOUR
T1 - Efficacy and Safety of Transcranial Magnetic Stimulation for Post-surgical Motor Strength Recovery in
Neuro-oncologic Patients: A Systematic Review
AU - Ranhel De Roxas
AU - Ana Gabriela Cabungcal
AU - Mia Patrice Dela Vega
AU - Marian Sheryl Milo
Y1 - 2026/05/18
PY - 2026
N1 - https://doi.org/10.11648/j.cmr.20261503.11
DO - 10.11648/j.cmr.20261503.11
T2 - Clinical Medicine Research
JF - Clinical Medicine Research
JO - Clinical Medicine Research
SP - 34
EP - 40
PB - Science Publishing Group
SN - 2326-9057
UR - https://doi.org/10.11648/j.cmr.20261503.11
AB - Background: Post-surgical motor deficits are a frequent complication in neuro-oncologic patients and can significantly affect functional recovery. Transcranial magnetic stimulation (TMS) has emerged as a potential therapeutic modality to facilitate motor rehabilitation. This systematic review examined the effectiveness and safety of TMS in promoting motor recovery following brain tumor surgery. Methods: A systematic review of four studies evaluating TMS for postoperative motor rehabilitation in patients with brain tumors was performed. Outcome measures included motor function assessments using the British Medical Research Council (BMRC) scale, Fugl-Meyer Assessment (FMA), and Karnofsky Performance Status (KPS), as well as the incidence of adverse events. Results: The effects of TMS on motor recovery were inconsistent across studies, with some demonstrating improvements in BMRC and FMA scores, while others reported limited therapeutic benefit. Overall, TMS was generally well tolerated, with only minimal adverse events documented. Conclusions: TMS may represent a safe and promising adjunctive intervention for postoperative motor recovery in brain tumor patients; however, the current evidence remains insufficient to establish definitive clinical benefit. Further large-scale prospective studies using standardized treatment protocols are necessary to clarify its therapeutic efficacy and long-term safety profile.
VL - 15
IS - 3
ER -
Institute for Neurosciences, St. Luke’s Medical Center, Taguig City, Philippines;Department of Neurosciences, Philippine General Hospital, Manila, Philippines
Institute for Neurosciences, St. Luke’s Medical Center, Taguig City, Philippines
Mia Patrice Dela Vega
Institute for Neurosciences, St. Luke’s Medical Center, Taguig City, Philippines;Department of Neurosciences, Philippine General Hospital, Manila, Philippines
Marian Sheryl Milo
Institute for Neurosciences, St. Luke’s Medical Center, Taguig City, Philippines
Roxas, R. D., Cabungcal, A. G., Vega, M. P. D., Milo, M. S. (2026). Efficacy and Safety of Transcranial Magnetic Stimulation for Post-surgical Motor Strength Recovery in
Neuro-oncologic Patients: A Systematic Review. Clinical Medicine Research, 15(3), 34-40. https://doi.org/10.11648/j.cmr.20261503.11
Roxas, R. D.; Cabungcal, A. G.; Vega, M. P. D.; Milo, M. S. Efficacy and Safety of Transcranial Magnetic Stimulation for Post-surgical Motor Strength Recovery in
Neuro-oncologic Patients: A Systematic Review. Clin. Med. Res.2026, 15(3), 34-40. doi: 10.11648/j.cmr.20261503.11
Roxas RD, Cabungcal AG, Vega MPD, Milo MS. Efficacy and Safety of Transcranial Magnetic Stimulation for Post-surgical Motor Strength Recovery in
Neuro-oncologic Patients: A Systematic Review. Clin Med Res. 2026;15(3):34-40. doi: 10.11648/j.cmr.20261503.11
@article{10.11648/j.cmr.20261503.11,
author = {Ranhel De Roxas and Ana Gabriela Cabungcal and Mia Patrice Dela Vega and Marian Sheryl Milo},
title = {Efficacy and Safety of Transcranial Magnetic Stimulation for Post-surgical Motor Strength Recovery in
Neuro-oncologic Patients: A Systematic Review},
journal = {Clinical Medicine Research},
volume = {15},
number = {3},
pages = {34-40},
doi = {10.11648/j.cmr.20261503.11},
url = {https://doi.org/10.11648/j.cmr.20261503.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.cmr.20261503.11},
abstract = {Background: Post-surgical motor deficits are a frequent complication in neuro-oncologic patients and can significantly affect functional recovery. Transcranial magnetic stimulation (TMS) has emerged as a potential therapeutic modality to facilitate motor rehabilitation. This systematic review examined the effectiveness and safety of TMS in promoting motor recovery following brain tumor surgery. Methods: A systematic review of four studies evaluating TMS for postoperative motor rehabilitation in patients with brain tumors was performed. Outcome measures included motor function assessments using the British Medical Research Council (BMRC) scale, Fugl-Meyer Assessment (FMA), and Karnofsky Performance Status (KPS), as well as the incidence of adverse events. Results: The effects of TMS on motor recovery were inconsistent across studies, with some demonstrating improvements in BMRC and FMA scores, while others reported limited therapeutic benefit. Overall, TMS was generally well tolerated, with only minimal adverse events documented. Conclusions: TMS may represent a safe and promising adjunctive intervention for postoperative motor recovery in brain tumor patients; however, the current evidence remains insufficient to establish definitive clinical benefit. Further large-scale prospective studies using standardized treatment protocols are necessary to clarify its therapeutic efficacy and long-term safety profile.},
year = {2026}
}
TY - JOUR
T1 - Efficacy and Safety of Transcranial Magnetic Stimulation for Post-surgical Motor Strength Recovery in
Neuro-oncologic Patients: A Systematic Review
AU - Ranhel De Roxas
AU - Ana Gabriela Cabungcal
AU - Mia Patrice Dela Vega
AU - Marian Sheryl Milo
Y1 - 2026/05/18
PY - 2026
N1 - https://doi.org/10.11648/j.cmr.20261503.11
DO - 10.11648/j.cmr.20261503.11
T2 - Clinical Medicine Research
JF - Clinical Medicine Research
JO - Clinical Medicine Research
SP - 34
EP - 40
PB - Science Publishing Group
SN - 2326-9057
UR - https://doi.org/10.11648/j.cmr.20261503.11
AB - Background: Post-surgical motor deficits are a frequent complication in neuro-oncologic patients and can significantly affect functional recovery. Transcranial magnetic stimulation (TMS) has emerged as a potential therapeutic modality to facilitate motor rehabilitation. This systematic review examined the effectiveness and safety of TMS in promoting motor recovery following brain tumor surgery. Methods: A systematic review of four studies evaluating TMS for postoperative motor rehabilitation in patients with brain tumors was performed. Outcome measures included motor function assessments using the British Medical Research Council (BMRC) scale, Fugl-Meyer Assessment (FMA), and Karnofsky Performance Status (KPS), as well as the incidence of adverse events. Results: The effects of TMS on motor recovery were inconsistent across studies, with some demonstrating improvements in BMRC and FMA scores, while others reported limited therapeutic benefit. Overall, TMS was generally well tolerated, with only minimal adverse events documented. Conclusions: TMS may represent a safe and promising adjunctive intervention for postoperative motor recovery in brain tumor patients; however, the current evidence remains insufficient to establish definitive clinical benefit. Further large-scale prospective studies using standardized treatment protocols are necessary to clarify its therapeutic efficacy and long-term safety profile.
VL - 15
IS - 3
ER -