Abstract
Background: Functional dyspepsia (FD) is the second most common functional gastrointestinal disorder, associated with significant morbidity and impaired quality of life. Duodenal eosinophilia has emerged as a key pathophysiological mechanism underlying FD. Montelukast, a cysteinyl leukotriene receptor antagonist, has shown efficacy in pediatric FD with duodenal eosinophilia, but evidence in adults remains absent. This study aimed to determine the clinical efficacy of montelukast in adult patients with functional dyspepsia and duodenal eosinophilia. Methods: A randomized, double-blind, placebo-controlled parallel group trial was conducted at the Department of Gastroenterology, Bangabandhu Sheikh Mujib Medical University (BSMMU), Dhaka, from December 2021 to July 2023. Seventy-six adults with Rome IV-diagnosed FD and duodenal eosinophil count greater than 22/5HPF were randomized into two groups of 38 each. Group A received montelukast 10 mg daily and Group B received an identical placebo for four weeks. Symptom severity was assessed using a 5-point Likert scale at baseline and on day 29. Results: The majority of participants (46.1%) were aged 20 to 30 years and most were female. At baseline, both groups were comparable in age, sex, eosinophil count and Likert scores. Following treatment, a positive clinical response was observed in 94.7% of the montelukast group compared with 39.5% in the placebo group (p<0.001). Significant improvements were noted across all four symptom components including postprandial fullness, early satiation, epigastric pain and epigastric burning. Conclusion: Montelukast produced significant symptomatic improvement in adult FD patients with duodenal eosinophilia. It may be prescribed as an adjunct to conventional therapy in this patient population.
|
Published in
|
International Journal of Gastroenterology (Volume 10, Issue 1)
|
|
DOI
|
10.11648/j.ijg.20261001.19
|
|
Page(s)
|
51-58 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2026. Published by Science Publishing Group
|
Keywords
Functional Dyspepsia, Montelukast, Rome IV Criteria, Likert Scale
1. Introduction
Dyspepsia, derived from the Greek words "dys" and "pepse," literally means difficult digestion. It is defined as chronic or recurrent pain or discomfort localized to the upper abdomen and may be accompanied by bloating, nausea, vomiting and belching
| [1] | Talley NJ, Vakil N. Practice Parameters Committe of the American College of Gastroenterology. Guidelines for the management of dyspepsia. Am J Gastroenterol. 2005; 100: 2324-37. |
[1]
. Major causes include peptic ulcer disease, gastroesophageal reflux disease, gastrointestinal malignancy and functional dyspepsia (FD)
| [1] | Talley NJ, Vakil N. Practice Parameters Committe of the American College of Gastroenterology. Guidelines for the management of dyspepsia. Am J Gastroenterol. 2005; 100: 2324-37. |
[1]
. Functional dyspepsia is characterized by upper abdominal symptoms occurring in the absence of any identifiable organic, systemic, or metabolic disease
| [2] | Miwa H, Oshima T, Tomita T, Fukui H, Kondo T, Yamasaki T, Watari J. Recent understanding of the pathophysiology of functional dyspepsia: role of the duodenum as the pathogenic center. Journal of Gastroenterology. 2019 Apr 1; 54(4): 305-11. |
[2]
. It is the second most prevalent functional gastrointestinal disorder after irritable bowel syndrome and carries a considerable burden of morbidity and healthcare utilization
| [3] | Drossman DA, Dumitrascu DL. Rome III: New standard for functional gastrointestinal disorders. Journal of gastrointestinal and liver diseases: JGLD. 2006 Sep 1; 15(3): 237-41. |
[3]
.
According to the Rome IV criteria established in 2016, FD is defined by the presence of one or more of four cardinal symptoms: postprandial fullness, early satiation, epigastric pain and epigastric burning, with symptom onset at least six months prior to diagnosis
| [4] | Stanghellini V, Chan FK, Hasler WL, Malagelada JR, Suzuki H, Tack J, Talley NJ. Gastroduodenal disorders. Gastroenterology. 2016 May 1; 150(6): 1380-92. |
[4]
. Rome IV classifies FD into two subtypes: postprandial distress syndrome (PDS), characterized by meal-induced symptoms and epigastric pain syndrome (EPS), characterized by pain or burning not necessarily related to meals
| [4] | Stanghellini V, Chan FK, Hasler WL, Malagelada JR, Suzuki H, Tack J, Talley NJ. Gastroduodenal disorders. Gastroenterology. 2016 May 1; 150(6): 1380-92. |
[4]
. In Bangladesh, the prevalence of FD has been reported at 8.3% in the general population and as high as 11% in rural communities
| [5] | Perveen I, Rahman MM, Saha M, Rahman MM, Hasan MQ. Prevalence of irritable bowel syndrome and functional dyspepsia, overlapping symptoms and associated factors in a general population of Bangladesh. Indian Journal of Gastroenterology. 2014 May; 33(3): 265-73. |
| [6] | Rahman MM, Ghoshal UC, Kibria MG, Sultana N, Yusuf MA, Nahar S, Ahmed F, Rowshon AH, Hasan M. Functional dyspepsia, peptic ulcer and Helicobacter pylori infection in a rural community of South Asia: an endoscopy-assisted household survey. Clinical and translational gastroenterology. 2021 Apr 1; 12(4): e00334. |
[5, 6]
.
Traditionally, FD was regarded as a motility disorder of the stomach. Over the past decade, however, evidence has shifted toward the duodenum as the central pathogenic site. The duodenum in FD patients demonstrates heightened sensitivity to luminal stimulants such as acid, bile, lipids and enteric bacteria and is characterized by low-grade mucosal inflammation and increased permeability
| [2] | Miwa H, Oshima T, Tomita T, Fukui H, Kondo T, Yamasaki T, Watari J. Recent understanding of the pathophysiology of functional dyspepsia: role of the duodenum as the pathogenic center. Journal of Gastroenterology. 2019 Apr 1; 54(4): 305-11. |
[2]
. Psychological and physical stress have been shown to further compromise duodenal mucosal integrity
| [2] | Miwa H, Oshima T, Tomita T, Fukui H, Kondo T, Yamasaki T, Watari J. Recent understanding of the pathophysiology of functional dyspepsia: role of the duodenum as the pathogenic center. Journal of Gastroenterology. 2019 Apr 1; 54(4): 305-11. |
[2]
.
Among the most consistent duodenal findings in FD is eosinophilia. Talley et al. conducted a landmark population-based case-control study in Swedish adults and demonstrated significantly elevated duodenal eosinophil counts in FD patients compared with controls, with early satiety most strongly associated with this finding
| [7] | Talley NJ, Walker MM, Aro P, Ronkainen J, Storskrubb T, Hindley LA, Harmsen WS, Zinsmeister AR, Agréus L. Non-ulcer dyspepsia and duodenal eosinophilia: an adult endoscopic population-based case-control study. Clinical Gastroenterology and Hepatology. 2007 Oct 1; 5(10): 1175-83. |
[7]
. Subsequent studies from the United Kingdom
| [8] | Walker MM, Salehian SS, Murray CE, Rajendran A, Hoare JM, Negus R, Powell N, Talley NJ. Implications of eosinophilia in the normal duodenal biopsy–an association with allergy and functional dyspepsia. Alimentary pharmacology & therapeutics. 2010 Jun; 31(11): 1229-36. |
[8]
, Japan
| [9] | Futagami S, Shindo T, Kawagoe T, Horie A, Shimpuku M, Gudis K, Iwakiri K, Itoh T, Sakamoto C. Migration of eosinophils and CCR2-/CD68-double positive cells into the duodenal mucosa of patients with postinfectious functional dyspepsia. Official journal of the American College of Gastroenterology| ACG. 2010 Aug 1; 105(8): 1835-42. |
[9]
, Australia
| [10] | Walker MM, Aggarwal KR, Shim LS, Bassan M, Kalantar JS, Weltman MD, Jones M, Powell N, Talley NJ. Duodenal eosinophilia and early satiety in functional dyspepsia: confirmation of a positive association in an A ustralian cohort. Journal of gastroenterology and hepatology. 2014 Mar; 29(3): 474-9. |
[10]
and Bangladesh
| [12] | Friesen CA, Kearns GL andre L, Neustrom M, Roberts CC, Abdel‐Rahman SM. Clinical efficacy and pharmacokinetics of montelukast in dyspeptic children with duodenal eosinophilia. Journal of pediatric gastroenterology and nutrition. 2004 Mar; 38(3): 343-51. |
[12]
have confirmed this association. Duodenal eosinophilia is defined as a peak count exceeding 22 eosinophils per 5 high-power fields (5HPF) in adults
| [7] | Talley NJ, Walker MM, Aro P, Ronkainen J, Storskrubb T, Hindley LA, Harmsen WS, Zinsmeister AR, Agréus L. Non-ulcer dyspepsia and duodenal eosinophilia: an adult endoscopic population-based case-control study. Clinical Gastroenterology and Hepatology. 2007 Oct 1; 5(10): 1175-83. |
[7]
. Eosinophils contribute to gastrointestinal symptoms by releasing chemical mediators that impair motility and heighten visceral sensitivity.
Montelukast is a selective antagonist of the type 1 cysteinyl leukotriene receptor (CysLT1), with affinity comparable to its natural ligand leukotriene D4. Its effects include reduced eosinophil density, altered eosinophil activation, inhibition of leukotriene-mediated signaling and decreased mucosal permeability
| [13] | Vanderhoof JA, Young RJ, Hanner TL, Kettlehut B. Montelukast: use in pediatric patients with eosinophilic gastrointestinal disease. Journal of pediatric gastroenterology and nutrition. 2003 Feb; 36(2): 293-4. |
[13]
. The drug has been used in other eosinophil-associated gastrointestinal conditions, including eosinophilic gastroenteritis
| [14] | Attwood SE, Lewis CJ, Bronder CS, Morris CD, Armstrong GR, Whittam J. Eosinophilic oesophagitis: a novel treatment using Montelukast. Gut. 2003 Feb 1; 52(2): 181-5. |
[14]
and eosinophilic esophagitis
| [15] | Friesen CA, Neilan NA, Schurman JV, Taylor DL, Kearns GL, Abdel-Rahman SM. Montelukast in the treatment of duodenal eosinophilia in children with dyspepsia: effect on eosinophil density and activation in relation to pharmacokinetics. BMC gastroenterology. 2009 May 11; 9(1): 32. |
[15]
, with favorable outcomes. In a randomized controlled trial involving children and adolescents with FD and duodenal eosinophilia, Friesen et al. reported a positive clinical response rate of 62.1% with montelukast versus 32.4% with placebo
| [13] | Vanderhoof JA, Young RJ, Hanner TL, Kettlehut B. Montelukast: use in pediatric patients with eosinophilic gastrointestinal disease. Journal of pediatric gastroenterology and nutrition. 2003 Feb; 36(2): 293-4. |
[13]
. A subsequent study by the same group found that 83% of pediatric patients with peak duodenal eosinophil counts above 20/HPF responded positively to montelukast, with 50% achieving near-complete or complete symptom relief
| [16] | Aziz I, Palsson OS, Törnblom H, Sperber AD, Whitehead WE, Simrén M. Epidemiology, clinical characteristics and associations for symptom-based Rome IV functional dyspepsia in adults in the USA, Canada and the UK: a cross-sectional population-based study. The lancet Gastroenterology & hepatology. 2018 Apr 1; 3(4): 252-62. |
[16]
.
Despite this evidence, no trial has evaluated the efficacy of montelukast in adult patients with FD and duodenal eosinophilia and no such study has been conducted in Bangladesh. This trial was designed to address that gap by assessing the clinical efficacy of montelukast across all four Rome IV symptom components and both FD subtypes in an adult population.
2. Methodology
2.1. Study Design and Setting
This was a randomized, double-blind, placebo-controlled parallel group clinical trial conducted at the Department of Gastroenterology, Bangabandhu Sheikh Mujib Medical University (BSMMU), Dhaka, Bangladesh. The study was carried out from December 2021 to July 2023. The study population comprised adult dyspeptic patients attending the Gastroenterology outpatient department of BSMMU who fulfilled the Rome IV diagnostic criteria for functional dyspepsia and had confirmed duodenal eosinophilia on histopathology.
2.2. Selection Criteria
2.2.1. Inclusion Criteria
(i) Diagnosis of functional dyspepsia (FD) based on the Rome IV
(ii) Duodenal mucosal biopsy showing no other pathology and a peak eosinophil count greater than 22/5HPF
(iii) Age between 18 and 55 years
(iv) willingness to participate and provision of written informed consent.
2.2.2. Exclusion Criteria
(i) Presence of alarm features including unintentional weight loss, progressive dysphagia, recurrent or persistent vomiting, evidence of gastrointestinal bleeding, or anemia
(ii) Previous treatment with montelukast
(iii) use of corticosteroids or oral cromolyn sodium within four weeks prior to enrollment
(iv) Any history, clinical signs, or biochemical evidence of hepatic or renal abnormality
(v) Exposure to drugs known to induce or inhibit cytochrome P-450 enzymes, including rifampicin, carbamazepine, phenobarbital, phenytoin, St. John's wort, fluconazole, paroxetine, azole antifungals, ciprofloxacin, clarithromycin, or erythromycin
(vi) Regular use of NSAIDs or aspirin
(vii) History of previous abdominal surgery
2.3. Sample Size and Randomization
Sample size was calculated using the standard formula for clinical trials, based on an expected positive response rate of 84% in the montelukast group and 42% in the placebo group, derived from a prior pediatric trial
| [13] | Vanderhoof JA, Young RJ, Hanner TL, Kettlehut B. Montelukast: use in pediatric patients with eosinophilic gastrointestinal disease. Journal of pediatric gastroenterology and nutrition. 2003 Feb; 36(2): 293-4. |
[13]
, at a 1% level of significance and 95% statistical power. This yielded a minimum of 38 participants per group, for a total of 76. Randomization was performed by lottery, with patients allocated to Group A (montelukast) or Group B (placebo) in equal numbers.
2.4. Study Procedure
Consecutive patients fulfilling the eligibility criteria underwent clinical history taking, physical examination and routine investigations including complete blood count, fasting glucose, serum electrolytes, alanine aminotransferase, serum creatinine, thyroid stimulating hormone, serum calcium and abdominal ultrasonography, to exclude organic causes of dyspepsia. Patients with normal investigation results proceeded to upper gastrointestinal endoscopy. Two standard biopsy specimens from the second part of the duodenum, fixed in 10% buffered formalin, were sent to the Department of Pathology, BSMMU, for histopathological evaluation by a single expert pathologist. A single antral biopsy was obtained for rapid urease testing for Helicobacter pylori; patients testing positive were excluded.
Seventy-six patients who met the histological criteria for duodenal eosinophilia were randomly allocated to Group A or Group B. Group A received montelukast 10 mg orally once daily for four weeks. Group B received a placebo tablet identical in size, shape, color and taste to the active drug (Aeron, montelukast 10 mg) for the same duration. Medications were labeled only as A or B, ensuring blinding of both patients and the investigator. Symptom severity was assessed on study day 1 using a validated 5-point Likert scale, where 1 indicated no problem and 5 indicated a very severe problem. On day 29, symptoms were reassessed using the same instrument. Positive clinical response was defined as a total score indicating overall symptomatic improvement. Symptom relief for individual components was defined as a post-treatment Likert score of 1 or 2 among patients who scored 3 or above at baseline. Patients returned medication strips at the end of treatment to verify compliance and any adverse effects were recorded at that visit.
2.5. Ethical Consideration
Ethical clearance was obtained from the Institutional Review Board (IRB) of BSMMU prior to study commencement. Written informed consent was obtained from all participants after explaining the study objectives, procedures, potential risks and benefits, in accordance with the Declaration of Helsinki. Confidentiality of all patient data was maintained throughout and participants were free to withdraw at any point without consequence. No conflicts of interest were declared.
2.6. Statistical Analysis
All collected data were checked and entered into SPSS (Statistical Package for the Social Sciences). Continuous variables were expressed as mean and standard deviation, while categorical variables were summarized as frequencies and percentages. The Shapiro-Wilk test was used to assess normality. Since the Likert scale data were not normally distributed, continuous variables were compared between groups using the Mann-Whitney U test. Categorical variables were analyzed using the chi-square test or Fisher's exact test, as appropriate. A p-value of less than 0.05 was considered statistically significant.
3. Results
Table 1. Distribution of the participants according to demographic characteristics (n=76).
Demographic characteristics | Group A (n=38) | Group B (n=38) | Total | P value |
Age (years) | 20-30 | 17 (44.7) | 18 (47.4) | 35 (46.1) | 0.881 |
31-40 | 13 (34.2) | 11 (28.9) | 24 (31.6) |
41-55 | 8 (21.1) | 9 (23.7) | 17 (22.4) |
Mean ± SD | 34.26±10.09 | 33.68±9.93 | 33.97±9.95 | 0.666 |
Gender | Male | 20 (52.6) | 17 (44.7) | 37 (48.7) | 0.491 |
Female | 18 (47.4) | 21 (55.3) | 39 (51.3) |
Table 1 presents the baseline demographic characteristics of the study participants. The mean age was 34.26±10.09 years in Group A and 33.68±9.93 years in Group B, with the majority of participants (46.1%) falling in the 20–30 year age group. The two groups were well-matched at baseline, with no statistically significant differences in age distribution or gender (p>0.05 for both).
Table 2. Distribution of the participants according to the subtypes of functional dyspepsia with their symptom components in group A and group B (n=76).
Presenting complains | | Group A (n=38) | Group B (n=38) | P value |
PDS (Post prandial distress syndrome) | Postprandial fullness | 37 (97.4) | 36 (94.7) | >0.99 |
Early satiation | 35 (92.1) | 35 (92.1) | >0.99 |
EPS (Epigastric pain syndrome) | Epigastric pain | 12 (28.9) | 19 (50.0) | 0.06 |
Epigastric burning | 14 (36.8) | 24 (60.5) | 0.039 |
Table 2 presents the distribution of FD subtypes and symptom components at baseline. Postprandial fullness and early satiation were similarly distributed between the two groups (p>0.99 for both). Epigastric burning was significantly more prevalent in Group B than in Group A (60.5% vs. 36.8%, p=0.039), while the difference in epigastric pain did not reach statistical significance (50.0% vs. 28.9%, p=0.060).
Table 3. Distribution of the duodenal eosinophil count (/5 HPF) among the study participants (n=76).
Eosinophil count (/5 HPF) | Group A | Group B | P value |
Mean ±SD | 39.42 ± 15.20 | 33.13 ± 10.69 | 0.062 |
Median (range) | 36 (22.0-85.0) | 30 (22.0-75.0) |
Table 3 presents the baseline duodenal eosinophil counts. The mean ±SD eosinophil count was 39.42±15.20/5HPF in Group A and 33.13±10.69/5HPF in Group B, with median values of 36 (range 22–85) and 30 (range 22–75), respectively. The two groups were comparable at baseline, with no statistically significant difference in eosinophil count (p=0.062).
Table 4. Comparison of individual symptom severity (Likert scale) before and after treatment between Group A and Group B.
Symptom | Group A (n=38) Mean ± SD | Group B (n=38) Mean ± SD | P value |
Postprandial fullness | Before treatment | 4.45 ± 0.80 | 4.18 ± 0.73 | 0.051 |
After treatment | 2.03 ± 0.49 | 4.02 ± 1.00 | <0.001 |
Early satiation | Before treatment | 4.26 ± 0.92 | 4.08 ± 0.85 | 0.179 |
After treatment | 1.89 ± 0.51 | 3.94 ± 1.04 | <0.001 |
Epigastric pain | Before treatment | 1.68 ± 1.16 | 2.18 ± 1.31 | 0.067 |
After treatment | 1.13 ± 0.34 | 2.00 ± 1.18 | <0.001 |
Epigastric burning | Before treatment | 1.95 ± 1.39 | 2.26 ± 1.16 | 0.146 |
After treatment | 1.29 ± 0.57 | 2.07 ± 1.12 | <0.001 |
Table 4 presents the Likert scale scores for individual symptom components before and after treatment. At baseline, the two groups were comparable across all four symptoms, with no statistically significant differences in postprandial fullness (4.45±0.80 vs. 4.18±0.73, p=0.051), early satiation (4.26±0.92 vs. 4.08±0.85, p=0.179), epigastric pain (1.68±1.16 vs. 2.18±1.31, p=0.067), or epigastric burning (1.95±1.39 vs. 2.26±1.16, p=0.146) between Group A and Group B.
Following four weeks of treatment, Group A demonstrated significant improvement in all four symptom components compared to Group B. Mean Likert scores for postprandial fullness (2.03±0.49 vs. 4.02±1.00), early satiation (1.89±0.51 vs. 3.94±1.04), epigastric pain (1.13±0.34 vs. 2.00±1.18) and epigastric burning (1.29±0.57 vs. 2.07±1.12) were all significantly lower in the montelukast group than in the placebo group (p<0.001 for all).
Table 5. Comparison of the Severity of Postprandial Distress Syndrome (PDS) and Epigastric Pain Syndrome (EPS) by Using the Likert Scale Score Between Two Groups.
Score | Group A (n=38) Mean ± SD | Group B (n=38) Mean ± SD | P value |
Postprandial Distress Syndrome (Abdominal fullness + Early satiety) | Before treatment | 8.71 ± 1.59 | 8.26 ± 1.45 | 0.101 |
After treatment | 3.92 ± 0.91 | 7.97 ± 1.81 | <0.001 |
Epigastric Pain Syndrome (Epigastric pain + Epigastric burning) | Before treatment | 3.63 ± 1.99 | 4.45 ± 2.15 | 0.082 |
After treatment | 2.42 ± 0.68 | 4.08 ± 2.10 | <0.001 |
Table 5 presents the Likert scale scores for FD syndrome subtypes before and after treatment. At baseline, PDS scores (8.71±1.59 vs. 8.26±1.45, p=0.101) and EPS scores (3.63±1.99 vs. 4.45±2.15, p=0.082) were comparable between Group A and Group B, with no statistically significant differences.
Following four weeks of treatment, Group A demonstrated significant improvement in both syndrome subtypes compared to Group B. Mean Likert scores for PDS (3.92±0.91 vs. 7.97±1.81) and EPS (2.42±0.68 vs. 4.08±2.10) were significantly lower in the montelukast group than in the placebo group (p<0.001 for both).
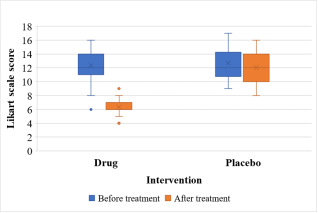
Figure 1. Box-plot of the distribution of Likert scale score of the symptoms before and after treatment in two groups.
Table 6. Comparison of severity of symptoms of functional dyspepsia by using the total Likert scale score between two groups.
Likert scale | Group A (n=38) | Group B (n=38) | P value |
Before treatment | Mean ± SD | 12.34 ± 2.29 | 12.71 ± 2.18 | 0.643 |
After treatment | Mean ± SD | 6.34 ± 1.15 | 12.05 ± 2.04 | <0.001 |
Table 6 presents the total FD Likert scale scores and overall clinical response. At baseline, total Likert scores were comparable between groups (12.34±2.29 vs. 12.71±2.18, p=0.643). Following treatment, the total score was significantly lower in Group A than in Group B (6.34±1.15 vs. 12.05±2.04, p<0.001). A positive clinical response was observed in 94.7% of patients in Group A compared with 39.5% in Group B (p<0.001).
Table 7. Distribution of overall outcome (improvement in terms of positive clinical response) between two groups.
Overall outcome | Group A (n=38) | Group B (n=38) | P value |
Improved | Frequency (%) | 36 (94.7) | 15 (39.5) | <0.001 |
Not improved | Frequency (%) | 2 (5.3) | 23 (60.5) |
Table 7 presents the overall clinical response in terms of positive response rate. A positive clinical response was observed in 94.7% of patients treated with montelukast compared with 39.5% in the placebo group, a difference that was statistically significant (p<0.001).
Table 8. Distribution of patients who achieved symptom relief after treatment.
Presenting complains of functional dyspepsia | Group A | Group B | P value |
PDS (Post prandial distress syndrome) | Postprandial fullness | 32 (86.5%) | 5 (13.9%) | <0.001 |
Early satiation | 32 (91.4%) | 4 (11.4%) | <0.001 |
EPS (Epigastric pain syndrome) | Epigastric pain | 8 (66.7%) | 5 (26.3%) | <0.027 |
Epigastric burning | 9 (64.3%) | 6 (25.0%) | <0.013 |
Table 8 presents symptom relief rates for each individual component of FD, defined as a post-treatment Likert score of 1 or 2 among patients who scored 3 or above at baseline. Symptom relief was significantly higher in Group A than Group B across all four components: postprandial fullness (86.5% vs. 13.9%), early satiation (91.4% vs. 11.4%), epigastric pain (66.7% vs. 26.3%) and epigastric burning (64.3% vs. 25.0%), with p<0.05 for all comparisons.
4. Discussion
Duodenal eosinophilia has been established as a consistent pathological finding in functional dyspepsia across multiple international and local studies
| [7] | Talley NJ, Walker MM, Aro P, Ronkainen J, Storskrubb T, Hindley LA, Harmsen WS, Zinsmeister AR, Agréus L. Non-ulcer dyspepsia and duodenal eosinophilia: an adult endoscopic population-based case-control study. Clinical Gastroenterology and Hepatology. 2007 Oct 1; 5(10): 1175-83. |
| [11] | Sarkar AM, Akhter S, Khan MR, Saha M, Alam MR, Ghosh CK, Ahmed DS, Miah AR, Roy PK. Evaluation of Duodenal Eosinophil Count in Adult Patients with Functional Dyspepsia. Mymensingh Medical Journal: MMJ. 2019 Jan 1; 28(1): 150-6. |
[7, 11]
. Montelukast, owing to its ability to antagonize cysteinyl leukotriene signaling and reduce eosinophil-driven mucosal inflammation, has been proposed as a targeted therapeutic option for this condition. Prior evidence supporting this approach was, however, limited to pediatric populations
| [12] | Friesen CA, Kearns GL andre L, Neustrom M, Roberts CC, Abdel‐Rahman SM. Clinical efficacy and pharmacokinetics of montelukast in dyspeptic children with duodenal eosinophilia. Journal of pediatric gastroenterology and nutrition. 2004 Mar; 38(3): 343-51. |
| [15] | Friesen CA, Neilan NA, Schurman JV, Taylor DL, Kearns GL, Abdel-Rahman SM. Montelukast in the treatment of duodenal eosinophilia in children with dyspepsia: effect on eosinophil density and activation in relation to pharmacokinetics. BMC gastroenterology. 2009 May 11; 9(1): 32. |
[12, 15]
. This trial is, to the best of the authors' knowledge, the first randomized controlled trial to evaluate the clinical efficacy of montelukast in adult patients with FD and confirmed duodenal eosinophilia.
The demographic profile of study participants was broadly consistent with established epidemiological data on FD. The majority of participants in both groups fell within the 20 to 30 year age bracket and females outnumbered males overall, a pattern consistent with findings from a large cross-sectional study of Rome IV FD in North America and the United Kingdom by Aziz et al.
| [16] | Aziz I, Palsson OS, Törnblom H, Sperber AD, Whitehead WE, Simrén M. Epidemiology, clinical characteristics and associations for symptom-based Rome IV functional dyspepsia in adults in the USA, Canada and the UK: a cross-sectional population-based study. The lancet Gastroenterology & hepatology. 2018 Apr 1; 3(4): 252-62. |
[16]
. Both groups were well-matched at baseline with respect to age and sex distribution, supporting the validity of between-group comparisons.
The mean duodenal eosinophil count was 39.42±15.20/5HPF in Group A and 33.13±10.69/5HPF in Group B, with no statistically significant difference between groups at baseline (p=0.062). These counts were notably higher than those reported by Sarkar et al. in a Bangladeshi cohort, where the mean count was 22.78±8.78/5HPF
| [12] | Friesen CA, Kearns GL andre L, Neustrom M, Roberts CC, Abdel‐Rahman SM. Clinical efficacy and pharmacokinetics of montelukast in dyspeptic children with duodenal eosinophilia. Journal of pediatric gastroenterology and nutrition. 2004 Mar; 38(3): 343-51. |
[12]
and were comparable to findings from Talley et al., who reported a mean of 34.6±16.9/5HPF in the second part of the duodenum among Swedish FD patients
| [7] | Talley NJ, Walker MM, Aro P, Ronkainen J, Storskrubb T, Hindley LA, Harmsen WS, Zinsmeister AR, Agréus L. Non-ulcer dyspepsia and duodenal eosinophilia: an adult endoscopic population-based case-control study. Clinical Gastroenterology and Hepatology. 2007 Oct 1; 5(10): 1175-83. |
[7]
. The cut-off of greater than 22/5HPF applied in the current study follows the widely accepted diagnostic threshold for duodenal eosinophilia in adults
| [7] | Talley NJ, Walker MM, Aro P, Ronkainen J, Storskrubb T, Hindley LA, Harmsen WS, Zinsmeister AR, Agréus L. Non-ulcer dyspepsia and duodenal eosinophilia: an adult endoscopic population-based case-control study. Clinical Gastroenterology and Hepatology. 2007 Oct 1; 5(10): 1175-83. |
[7]
. In comparison, the pediatric trials by Friesen et al. used a lower threshold of greater than 10/HPF and 20/HPF respectively
| [12] | Friesen CA, Kearns GL andre L, Neustrom M, Roberts CC, Abdel‐Rahman SM. Clinical efficacy and pharmacokinetics of montelukast in dyspeptic children with duodenal eosinophilia. Journal of pediatric gastroenterology and nutrition. 2004 Mar; 38(3): 343-51. |
| [15] | Friesen CA, Neilan NA, Schurman JV, Taylor DL, Kearns GL, Abdel-Rahman SM. Montelukast in the treatment of duodenal eosinophilia in children with dyspepsia: effect on eosinophil density and activation in relation to pharmacokinetics. BMC gastroenterology. 2009 May 11; 9(1): 32. |
[12, 15]
, reflecting the inherently different mucosal eosinophil distribution in younger age groups.
A key methodological strength of the present study is its comprehensive symptom assessment framework. Unlike the pediatric trials by Friesen et al.
| [12] | Friesen CA, Kearns GL andre L, Neustrom M, Roberts CC, Abdel‐Rahman SM. Clinical efficacy and pharmacokinetics of montelukast in dyspeptic children with duodenal eosinophilia. Journal of pediatric gastroenterology and nutrition. 2004 Mar; 38(3): 343-51. |
| [15] | Friesen CA, Neilan NA, Schurman JV, Taylor DL, Kearns GL, Abdel-Rahman SM. Montelukast in the treatment of duodenal eosinophilia in children with dyspepsia: effect on eosinophil density and activation in relation to pharmacokinetics. BMC gastroenterology. 2009 May 11; 9(1): 32. |
[12, 15]
, which assessed only pain using a global relief scale, this study quantified all four Rome IV symptom components including postprandial fullness, early satiation, epigastric pain and epigastric burning, along with the composite PDS and EPS subscores, using a validated 5-point Likert scale before and after treatment. This approach provides a more complete and clinically meaningful picture of treatment response and aligns with current standards for FD assessment.
At baseline, total Likert scores were comparable between the two groups (12.34±2.29 vs. 12.71±2.18, p=0.643). Following four weeks of treatment, scores declined markedly in Group A while remaining essentially unchanged in Group B, with a highly significant between-group difference (6.34±1.15 vs. 12.05±2.04, p<0.001). A positive clinical response was observed in 94.7% of patients in the montelukast group compared with 39.5% in the placebo group. This response rate exceeds those previously reported by Friesen et al. in 2004 (62.1% vs. 32.4%, p<0.02)
| [12] | Friesen CA, Kearns GL andre L, Neustrom M, Roberts CC, Abdel‐Rahman SM. Clinical efficacy and pharmacokinetics of montelukast in dyspeptic children with duodenal eosinophilia. Journal of pediatric gastroenterology and nutrition. 2004 Mar; 38(3): 343-51. |
[12]
and in 2009 (83% positive response)
| [15] | Friesen CA, Neilan NA, Schurman JV, Taylor DL, Kearns GL, Abdel-Rahman SM. Montelukast in the treatment of duodenal eosinophilia in children with dyspepsia: effect on eosinophil density and activation in relation to pharmacokinetics. BMC gastroenterology. 2009 May 11; 9(1): 32. |
[15]
, though direct comparison is limited by differences in study population, eosinophil thresholds and outcome assessment tools.
Symptom-level analysis further confirmed the breadth of montelukast's efficacy. Symptom relief rates in Group A were significantly higher than in Group B across all four components: postprandial fullness (86.5% vs. 13.9%), early satiation (91.4% vs. 11.4%), epigastric pain (66.7% vs. 26.3%) and epigastric burning (64.3% vs. 25.0%), with p<0.05 for all comparisons. The most pronounced improvement was observed in early satiation and postprandial fullness, both of which are hallmark features of PDS and have been consistently linked with duodenal eosinophilia in prior studies
| [7] | Talley NJ, Walker MM, Aro P, Ronkainen J, Storskrubb T, Hindley LA, Harmsen WS, Zinsmeister AR, Agréus L. Non-ulcer dyspepsia and duodenal eosinophilia: an adult endoscopic population-based case-control study. Clinical Gastroenterology and Hepatology. 2007 Oct 1; 5(10): 1175-83. |
| [8] | Walker MM, Salehian SS, Murray CE, Rajendran A, Hoare JM, Negus R, Powell N, Talley NJ. Implications of eosinophilia in the normal duodenal biopsy–an association with allergy and functional dyspepsia. Alimentary pharmacology & therapeutics. 2010 Jun; 31(11): 1229-36. |
[7, 8]
. Statistically significant improvement was also observed in EPS components, namely epigastric pain and burning. This is particularly noteworthy because EPS is conventionally managed with acid-suppressive therapy, while PDS responds to prokinetic agents
| [17] | Miwa H, Kusano M, Arisawa T, Oshima T, Kato M, Joh T, Suzuki H, Tominaga K, Nakada K, Nagahara A, Futagami S. Evidence-based clinical practice guidelines for functional dyspepsia. Journal of gastroenterology. 2015 Feb; 50(2): 125-39. |
[17]
. The significant response in both subtypes observed in the present study suggests that targeting the eosinophilic inflammatory pathway with montelukast may offer broader therapeutic coverage than currently available treatment strategies.
The overall magnitude and consistency of improvement across FD subtypes in this adult trial lends clinical weight to the mechanistic rationale for using montelukast in this context. Taken together with the findings of Friesen et al.
| [12] | Friesen CA, Kearns GL andre L, Neustrom M, Roberts CC, Abdel‐Rahman SM. Clinical efficacy and pharmacokinetics of montelukast in dyspeptic children with duodenal eosinophilia. Journal of pediatric gastroenterology and nutrition. 2004 Mar; 38(3): 343-51. |
| [15] | Friesen CA, Neilan NA, Schurman JV, Taylor DL, Kearns GL, Abdel-Rahman SM. Montelukast in the treatment of duodenal eosinophilia in children with dyspepsia: effect on eosinophil density and activation in relation to pharmacokinetics. BMC gastroenterology. 2009 May 11; 9(1): 32. |
[12, 15]
, the present results support consideration of montelukast as an adjunctive treatment option for adult patients with FD and confirmed duodenal eosinophilia.
5. Limitations
1) It was a single center-based study.
2) The sample size of the study was small.
3) The Likert scale used for assessment of symptomatic improvement and thus efficacy of montelukast is a subjective scale. So, there is a chance of bias from patients’ perspectives while answering according to the scale.
4) Duodenal eosinophil count was not measured after being treated with montelukast or a placebo.
5) Long-term efficacy of montelukast in functional dyspepsia was not assessed in this study.
6. Conclusion
This randomized controlled trial demonstrates that montelukast produces significant and clinically meaningful symptomatic improvement in adult patients with functional dyspepsia and duodenal eosinophilia. A positive clinical response was observed in nearly 95% of treated patients, with significant improvement across all four Rome IV symptom components and both PDS and EPS subtypes. These findings extend prior pediatric evidence to the adult population for the first time and suggest that montelukast may serve as a viable adjunct to conventional FD management in patients with confirmed duodenal eosinophilia. Multicenter trials with larger sample sizes, post-treatment histological evaluation and longer follow-up periods are warranted to further establish its role in clinical practice.
Abbreviations
BSMMU | Bangabandhu Sheikh Mujib Medical University |
EPS | Epigastric Pain Syndrome |
FD | Functional Dyspepsia |
IRB | Institutional Review Board |
NSAIDs | Nonsteroidal Anti-Inflammatory Drugs |
PDS | Postprandial Distress Syndrome |
SPSS | Statistical Package for the Social Sciences |
Author Contributions
Priyabrata Roy: Conceptualization, Resources, Writing – original draft, Writing – review & editing
Sampurna Sen: Conceptualization, Resources
Razibul Alam: Conceptualization, Resources
Muhammad Ataul Gani Osmani: Data curation, Methodology
Mosharraf Hossain: Data curation, Methodology
Antora Rahut: Data curation, Methodology
Abu Hena Shahinujjaman: Formal Analysis, Investigation
Conflicts of Interest
There are no conflicts of interest.
References
| [1] |
Talley NJ, Vakil N. Practice Parameters Committe of the American College of Gastroenterology. Guidelines for the management of dyspepsia. Am J Gastroenterol. 2005; 100: 2324-37.
|
| [2] |
Miwa H, Oshima T, Tomita T, Fukui H, Kondo T, Yamasaki T, Watari J. Recent understanding of the pathophysiology of functional dyspepsia: role of the duodenum as the pathogenic center. Journal of Gastroenterology. 2019 Apr 1; 54(4): 305-11.
|
| [3] |
Drossman DA, Dumitrascu DL. Rome III: New standard for functional gastrointestinal disorders. Journal of gastrointestinal and liver diseases: JGLD. 2006 Sep 1; 15(3): 237-41.
|
| [4] |
Stanghellini V, Chan FK, Hasler WL, Malagelada JR, Suzuki H, Tack J, Talley NJ. Gastroduodenal disorders. Gastroenterology. 2016 May 1; 150(6): 1380-92.
|
| [5] |
Perveen I, Rahman MM, Saha M, Rahman MM, Hasan MQ. Prevalence of irritable bowel syndrome and functional dyspepsia, overlapping symptoms and associated factors in a general population of Bangladesh. Indian Journal of Gastroenterology. 2014 May; 33(3): 265-73.
|
| [6] |
Rahman MM, Ghoshal UC, Kibria MG, Sultana N, Yusuf MA, Nahar S, Ahmed F, Rowshon AH, Hasan M. Functional dyspepsia, peptic ulcer and Helicobacter pylori infection in a rural community of South Asia: an endoscopy-assisted household survey. Clinical and translational gastroenterology. 2021 Apr 1; 12(4): e00334.
|
| [7] |
Talley NJ, Walker MM, Aro P, Ronkainen J, Storskrubb T, Hindley LA, Harmsen WS, Zinsmeister AR, Agréus L. Non-ulcer dyspepsia and duodenal eosinophilia: an adult endoscopic population-based case-control study. Clinical Gastroenterology and Hepatology. 2007 Oct 1; 5(10): 1175-83.
|
| [8] |
Walker MM, Salehian SS, Murray CE, Rajendran A, Hoare JM, Negus R, Powell N, Talley NJ. Implications of eosinophilia in the normal duodenal biopsy–an association with allergy and functional dyspepsia. Alimentary pharmacology & therapeutics. 2010 Jun; 31(11): 1229-36.
|
| [9] |
Futagami S, Shindo T, Kawagoe T, Horie A, Shimpuku M, Gudis K, Iwakiri K, Itoh T, Sakamoto C. Migration of eosinophils and CCR2-/CD68-double positive cells into the duodenal mucosa of patients with postinfectious functional dyspepsia. Official journal of the American College of Gastroenterology| ACG. 2010 Aug 1; 105(8): 1835-42.
|
| [10] |
Walker MM, Aggarwal KR, Shim LS, Bassan M, Kalantar JS, Weltman MD, Jones M, Powell N, Talley NJ. Duodenal eosinophilia and early satiety in functional dyspepsia: confirmation of a positive association in an A ustralian cohort. Journal of gastroenterology and hepatology. 2014 Mar; 29(3): 474-9.
|
| [11] |
Sarkar AM, Akhter S, Khan MR, Saha M, Alam MR, Ghosh CK, Ahmed DS, Miah AR, Roy PK. Evaluation of Duodenal Eosinophil Count in Adult Patients with Functional Dyspepsia. Mymensingh Medical Journal: MMJ. 2019 Jan 1; 28(1): 150-6.
|
| [12] |
Friesen CA, Kearns GL andre L, Neustrom M, Roberts CC, Abdel‐Rahman SM. Clinical efficacy and pharmacokinetics of montelukast in dyspeptic children with duodenal eosinophilia. Journal of pediatric gastroenterology and nutrition. 2004 Mar; 38(3): 343-51.
|
| [13] |
Vanderhoof JA, Young RJ, Hanner TL, Kettlehut B. Montelukast: use in pediatric patients with eosinophilic gastrointestinal disease. Journal of pediatric gastroenterology and nutrition. 2003 Feb; 36(2): 293-4.
|
| [14] |
Attwood SE, Lewis CJ, Bronder CS, Morris CD, Armstrong GR, Whittam J. Eosinophilic oesophagitis: a novel treatment using Montelukast. Gut. 2003 Feb 1; 52(2): 181-5.
|
| [15] |
Friesen CA, Neilan NA, Schurman JV, Taylor DL, Kearns GL, Abdel-Rahman SM. Montelukast in the treatment of duodenal eosinophilia in children with dyspepsia: effect on eosinophil density and activation in relation to pharmacokinetics. BMC gastroenterology. 2009 May 11; 9(1): 32.
|
| [16] |
Aziz I, Palsson OS, Törnblom H, Sperber AD, Whitehead WE, Simrén M. Epidemiology, clinical characteristics and associations for symptom-based Rome IV functional dyspepsia in adults in the USA, Canada and the UK: a cross-sectional population-based study. The lancet Gastroenterology & hepatology. 2018 Apr 1; 3(4): 252-62.
|
| [17] |
Miwa H, Kusano M, Arisawa T, Oshima T, Kato M, Joh T, Suzuki H, Tominaga K, Nakada K, Nagahara A, Futagami S. Evidence-based clinical practice guidelines for functional dyspepsia. Journal of gastroenterology. 2015 Feb; 50(2): 125-39.
|
Cite This Article
-
APA Style
Roy, P., Sen, S., Alam, R., Osmani, M. A. G., Hossain, M., et al. (2026). Clinical Efficacy of Montelukast on Functional Dyspepsia Patients with Duodenal Eosinophilia: A Double-Blind Placebo Controlled Trial. International Journal of Gastroenterology, 10(1), 51-58. https://doi.org/10.11648/j.ijg.20261001.19
 Copy
|
Copy
|
 Download
Download
ACS Style
Roy, P.; Sen, S.; Alam, R.; Osmani, M. A. G.; Hossain, M., et al. Clinical Efficacy of Montelukast on Functional Dyspepsia Patients with Duodenal Eosinophilia: A Double-Blind Placebo Controlled Trial. Int. J. Gastroenterol. 2026, 10(1), 51-58. doi: 10.11648/j.ijg.20261001.19
Copy
|
Download
AMA Style
Roy P, Sen S, Alam R, Osmani MAG, Hossain M, et al. Clinical Efficacy of Montelukast on Functional Dyspepsia Patients with Duodenal Eosinophilia: A Double-Blind Placebo Controlled Trial. Int J Gastroenterol. 2026;10(1):51-58. doi: 10.11648/j.ijg.20261001.19
Copy
|
Download
-
@article{10.11648/j.ijg.20261001.19,
author = {Priyabrata Roy and Sampurna Sen and Razibul Alam and Muhammad Ataul Gani Osmani and Mosharraf Hossain and Antora Rahut and Abu Hena Shahinujjaman},
title = {Clinical Efficacy of Montelukast on Functional Dyspepsia Patients with Duodenal Eosinophilia: A Double-Blind Placebo Controlled Trial},
journal = {International Journal of Gastroenterology},
volume = {10},
number = {1},
pages = {51-58},
doi = {10.11648/j.ijg.20261001.19},
url = {https://doi.org/10.11648/j.ijg.20261001.19},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijg.20261001.19},
abstract = {Background: Functional dyspepsia (FD) is the second most common functional gastrointestinal disorder, associated with significant morbidity and impaired quality of life. Duodenal eosinophilia has emerged as a key pathophysiological mechanism underlying FD. Montelukast, a cysteinyl leukotriene receptor antagonist, has shown efficacy in pediatric FD with duodenal eosinophilia, but evidence in adults remains absent. This study aimed to determine the clinical efficacy of montelukast in adult patients with functional dyspepsia and duodenal eosinophilia. Methods: A randomized, double-blind, placebo-controlled parallel group trial was conducted at the Department of Gastroenterology, Bangabandhu Sheikh Mujib Medical University (BSMMU), Dhaka, from December 2021 to July 2023. Seventy-six adults with Rome IV-diagnosed FD and duodenal eosinophil count greater than 22/5HPF were randomized into two groups of 38 each. Group A received montelukast 10 mg daily and Group B received an identical placebo for four weeks. Symptom severity was assessed using a 5-point Likert scale at baseline and on day 29. Results: The majority of participants (46.1%) were aged 20 to 30 years and most were female. At baseline, both groups were comparable in age, sex, eosinophil count and Likert scores. Following treatment, a positive clinical response was observed in 94.7% of the montelukast group compared with 39.5% in the placebo group (p Conclusion: Montelukast produced significant symptomatic improvement in adult FD patients with duodenal eosinophilia. It may be prescribed as an adjunct to conventional therapy in this patient population.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - Clinical Efficacy of Montelukast on Functional Dyspepsia Patients with Duodenal Eosinophilia: A Double-Blind Placebo Controlled Trial
AU - Priyabrata Roy
AU - Sampurna Sen
AU - Razibul Alam
AU - Muhammad Ataul Gani Osmani
AU - Mosharraf Hossain
AU - Antora Rahut
AU - Abu Hena Shahinujjaman
Y1 - 2026/05/21
PY - 2026
N1 - https://doi.org/10.11648/j.ijg.20261001.19
DO - 10.11648/j.ijg.20261001.19
T2 - International Journal of Gastroenterology
JF - International Journal of Gastroenterology
JO - International Journal of Gastroenterology
SP - 51
EP - 58
PB - Science Publishing Group
SN - 2640-169X
UR - https://doi.org/10.11648/j.ijg.20261001.19
AB - Background: Functional dyspepsia (FD) is the second most common functional gastrointestinal disorder, associated with significant morbidity and impaired quality of life. Duodenal eosinophilia has emerged as a key pathophysiological mechanism underlying FD. Montelukast, a cysteinyl leukotriene receptor antagonist, has shown efficacy in pediatric FD with duodenal eosinophilia, but evidence in adults remains absent. This study aimed to determine the clinical efficacy of montelukast in adult patients with functional dyspepsia and duodenal eosinophilia. Methods: A randomized, double-blind, placebo-controlled parallel group trial was conducted at the Department of Gastroenterology, Bangabandhu Sheikh Mujib Medical University (BSMMU), Dhaka, from December 2021 to July 2023. Seventy-six adults with Rome IV-diagnosed FD and duodenal eosinophil count greater than 22/5HPF were randomized into two groups of 38 each. Group A received montelukast 10 mg daily and Group B received an identical placebo for four weeks. Symptom severity was assessed using a 5-point Likert scale at baseline and on day 29. Results: The majority of participants (46.1%) were aged 20 to 30 years and most were female. At baseline, both groups were comparable in age, sex, eosinophil count and Likert scores. Following treatment, a positive clinical response was observed in 94.7% of the montelukast group compared with 39.5% in the placebo group (p Conclusion: Montelukast produced significant symptomatic improvement in adult FD patients with duodenal eosinophilia. It may be prescribed as an adjunct to conventional therapy in this patient population.
VL - 10
IS - 1
ER -
Copy
|
Download