Background: Although there are several clinical studies available regarding the management of bacterial infections, there is a dearth of studies among clinical experts on their practice. The survey aimed to assess clinical preferences and decision-making factors among clinicians regarding the use of co-amoxiclav and cefuroxime across a range of common infections and surgical indications in routine clinical practice in Indian settings. Methodology: This cross-sectional study was conducted among clinicians across India using a 22-item structured questionnaire. The questionnaire assessed common infection types, antibiotic usage patterns, indications for co-amoxiclav and cefuroxime, preferred regimens for community-acquired pneumonia (CAP), skin and soft tissue infections, and surgical prophylaxis, perceived comparative efficacy, factors influencing antibiotic choice, adverse drug reactions, and clinical outcomes using a global improvement scale. The data were analyzed using descriptive statistics. Results: Approximately 49% of clinicians identified streptococcal pharyngitis as the most common indication for recommending co-amoxiclav in routine practice. Nearly 60% reported co-amoxiclav as the most preferred empiric antimicrobial therapy for adult CAP in patients without comorbidities, while about 51% preferred it in patients with comorbidities. Around 76% of clinicians favored co-amoxiclav, with or without clindamycin, for the management of mild to moderate cellulitis in diabetic patients. Approximately 41% reported cefuroxime as the preferred prophylactic antibiotic for minimal access or laparoscopic surgeries, and about 37% highlighted long-duration sequential prophylaxis as its key advantage. Nearly 43% of respondents considered co-amoxiclav and cefuroxime to be equally effective for respiratory tract infections. About 66% of clinicians identified bacterial susceptibility as the most important factor influencing the choice between co-amoxiclav and cefuroxime. Conclusion: Co-amoxiclav is the preferred empiric antibiotic for streptococcal pharyngitis, CAP, and diabetic cellulitis, while cefuroxime remains the agent of choice for surgical prophylaxis in laparoscopic procedures. Bacterial susceptibility is the primary factor guiding antibiotic selection. The favorable safety profile and positive patient outcomes associated with co-amoxiclav support its continued role as a cornerstone agent in the empiric management of community-acquired infections in routine clinical practice.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
The global burden of infectious diseases remains substantial and is disproportionately higher in low- and lower-middle-income countries (LMICs) compared with high-income countries, where noncommunicable diseases account for most deaths. In 2019, infectious diseases caused approximately 7 million deaths worldwide, representing nearly 12% of global mortality. In addition, around 700,000 deaths occur annually due to infections caused by drug-resistant organisms, a number projected to rise to 10 million deaths per year by 2050 if effective control measures are not implemented. This growing burden is expected to result in economic losses of up to $100 trillion, with a disproportionate impact on LMICs.
[1]
Bhattarai S, Sharma BK, Subedi N, Ranabhat S, Baral MP. Burden of Serious Bacterial Infections and Multidrug-Resistant Organisms in an Adult Population of Nepal: A Comparative Analysis of Minimally Invasive Tissue Sampling Informed Mortality Surveillance of Community and Hospital Deaths. Clin Infect Dis. 2021; 73(Suppl_5): S415–21.
In India, infectious diseases continue to impose significant health and economic burdens, with the financial impact varying considerably across socioeconomic groups.
[2]
Ram B, Thakur R. Epidemiology and Economic Burden of Continuing Challenge of Infectious Diseases in India: Analysis of Socio-Demographic Differentials. Front Public Health. 2022; 10: 901276.
Respiratory infections represent a major share of this burden. In 2019, an estimated 17.2 billion incident cases of upper respiratory infections were reported globally, accounting for approximately 43% of all disease cases in the Global Burden of Disease study.
[3]
Jin X, Ren J, Li R, Gao Y, Zhang H, Li J, et al. Global burden of upper respiratory infections in 204 countries and territories, from 1990 to 2019. EClinicalMedicine. 2021; 37: 100986.
Lower respiratory infections (LRIs) were the leading cause of death from infectious diseases worldwide in 2019.
[4]
GBD 2021 Lower Respiratory Infections and Antimicrobial Resistance Collaborators. Global, regional, and national incidence and mortality burden of non-COVID-19 lower respiratory infections and aetiologies, 1990-2021: a systematic analysis from the Global Burden of Disease Study 2021. Lancet Infect Dis. 2024; 24(9): 974–1002.
In addition, surgical site infections remain important postoperative complications globally and are a major reason for the routine use of perioperative antibiotics. Appropriate selection of prophylactic antibiotics is therefore a critical component in the management of patients undergoing invasive surgical procedures.
[5]
Sastry GL, Nandi M, Mukhopadhyay M, Dumbre R, Bhattacharjee S, Sukumar G, et al. Role of cefuroxime as antibiotic prophylaxis for general surgery: An expert opinion. IP Journal of Surgery and Allied Sciences. 2025; 3(3): 58–71.
Amoxicillin/clavulanate (co-amoxiclav) is a combination antibiotic consisting of the semisynthetic penicillin amoxicillin and the β-lactamase inhibitor clavulanate potassium. Oral co-amoxiclav is a cornerstone antibiotic in community healthcare settings and is widely prescribed for the treatment of a broad range of infections. Multiple formulations are available for both adult and pediatric patients across different regions. Moreover, co-amoxiclav is the only oral penicillin formulation that includes a β-lactamase inhibitor. The drug was developed in response to increasing resistance to amoxicillin caused by β-lactamase–producing bacterial strains, a challenge overcome through the addition of clavulanic acid.
[6]
Jena D, Kanti Ghosh T, Pal A, Pawar D, Sharma A. Exploring the Therapeutic Potential of High Dose Co-amoxiclav (1 gm) in Different Clinical Conditions: A Review. Cureus. 2024; 16(7): e64717.
Choudhury J, Makkar A, Sharma V, Karamath SP, Parmar V, Kumar J P, et al. A Real-World Perspective of Co-amoxiclav Prescription Pattern with Probiotics for Pediatric Patients with Respiratory Tract Infections: Results of Quantitative and Qualitative Approach in Indian Outpatient Settings. Cureus. 2023; 15(3): e36269.
Cefuroxime is a second-generation cephalosporin antibiotic classified as a β-lactam agent. Approved by the U.S. Food and Drug Administration (FDA) in December 1987, it exhibits broad-spectrum activity against both Gram-positive and Gram-negative organisms, enabling effective treatment of a wide range of bacterial infections. Cefuroxime is commonly used for empirical therapy in community-acquired infections, including upper and lower respiratory tract infections, genitourinary tract infections, skin and soft tissue infections, and Lyme disease.
[8]
Omole AE, Awosika AO, Patel P. Cefuroxime. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 [cited 2026 Mar 7]. Available from:
In Indian healthcare settings, where infectious diseases remain a significant cause of morbidity, clinicians frequently manage a diverse range of bacterial infections across both outpatient and inpatient settings. The choice of empiric antimicrobial therapy often depends on clinical judgment supported by local antibiograms and evolving resistance patterns. However, limited data are available on clinicians’ preferences and decision-making factors regarding commonly used antibiotics such as co-amoxiclav and cefuroxime. The present survey aims to assess the treatment preferences and clinical practices of Indian clinicians with respect to the use of co-amoxiclav and cefuroxime in the management of common infectious conditions.
2. Materials and Methods
2.1. Study Settings
A cross-sectional study was carried out among clinicians involved in the management of bacterial infections in the major Indian cities from June 2025 to December 2025. The study was performed in accordance with Bangalore Ethics, an Independent Ethics Committee (ECR/355/Indt/KA/2022), which was recognized by the Indian Regulatory Authority, the Drug Controller General of India.
2.2. Study Participants
An invitation was sent to leading clinicians in managing bacterial infections in the month of March 2025 for participation in this Indian survey. About 1,067 clinicians from major cities of all Indian states, representing the geographical distribution, shared their willingness to participate and provide necessary data.
2.3. Study Procedure
The questionnaire booklet titled the RACE (Choosing the Right Antibiotic: Experts' Perspectives on Co-Amoxiclav and Cefuroxime and Managing Common Infections) was sent to the clinicians who were interested in participating in the survey. The study questionnaire comprised 22 questions that assessed multiple dimensions of bacterial infection management. The survey assessed commonly encountered infections, antibiotic usage practices (empiric versus culture-guided), and clinical indications for co-amoxiclav and cefuroxime. It also explored clinicians’ preferred treatment regimens for community-acquired pneumonia (CAP), skin and soft tissue infections, and the use of antibiotics for surgical prophylaxis. In addition, the questionnaire evaluated perceived comparative efficacy of the two antibiotics, key factors influencing antibiotic selection such as bacterial susceptibility and patient tolerance, reported adverse drug reactions, and treatment outcomes assessed using a global improvement scale. Reliability, as determined by a split-half test (coefficient alpha), was adequate but should be improved in future versions of the questionnaire. A study of criterion validity was undertaken to test the questionnaire and to develop methods of testing the validity of measures of clinicians' Perspectives. However, the extraneous variables in this include the clinician's experience, usage of the newer drugs, etc. The two criteria used were the doctors' perspectives from the clinical practice and the assessment of an external assessor and statistician. Clinicians had the option to skip questions as desired and were instructed to complete the survey independently, without peer consultation. Before participating in the survey, all respondents provided written informed consent.
2.4. Statistical Analysis
The data were analyzed using descriptive statistics, with categorical variables expressed as percentages to illustrate their distribution. Each variable’s frequency and corresponding percentage were reported to provide a comprehensive overview. To visually represent the distribution of categorical variables, pie and bar charts were generated using Microsoft Excel, version 2409, build 16.0.18025.20030.
3. Results
A total of 1,067 clinicians participated in the survey. The majority (80%) reported that respiratory infections are the most commonly encountered infections in their clinical practice. About 45% of experts indicated that they often recommend antibiotics based on local antibiogram data, reflecting the routine integration of resistance patterns into clinical decision-making. Similarly, around 44% reported that they often initiate empiric antibiotic therapy before culture results are available. Approximately 43% of participants indicated that they very often use amoxicillin as empiric therapy for suspected gram-positive infections. Nearly 45% identified Streptococcus pneumoniae as the most commonly encountered organism in Gram-positive infections in their clinical practice. According to 78% of clinicians, antibiotic resistance is the most common challenge encountered while prescribing antibiotics in routine clinical practice.
Approximately 48% of clinicians indicated that switching to a broader-spectrum antibiotic is their preferred approach when patients fail to respond to initial antibiotic therapy. Nearly half (51%) of clinicians reported occasionally encountering multidrug-resistant bacterial infections in routine clinical practice.
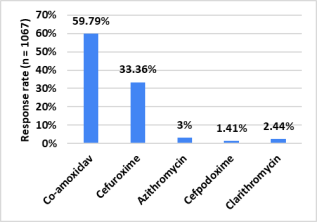
Around 49% indicated that streptococcal pharyngitis is the most common indication for recommending co-amoxiclav in routine practice (Table 1). About 60% of experts reported co-amoxiclav as their most preferred empiric antimicrobial therapy for adult CAP in patients without comorbidities (Figure 1). In patients with comorbidities, 51% of respondents favored co-amoxiclav as empiric antimicrobial therapy (Table 2). Additionally, 64% of participants reported that co-amoxiclav combined with a macrolide or doxycycline is the preferred empiric therapy for adult CAP patients admitted to non-ICU settings.
Table 1. Distribution of responses to common indications for which co-amoxiclav is recommended in clinical practice.
Indication
Response, N (%)
Streptococcal pharyngitis
522 (48.92%)
Bacterial sinusitis
198 (18.56%)
Acute otitis media
35 (3.28%)
Community-acquired pneumonia
36 (3.37%)
Cellulitis
0 (0%)
All of the above
276 (25.87%)
Table 2. Distribution of responses to preferred empiric antimicrobial therapy for adult CAP patients with comorbidities.
Figure 1. Distribution of responses to preferred empiric antimicrobial therapy for adult CAP without comorbidities.
Nearly 48% of clinicians preferred a 7-day course of antibiotic therapy for managing uncomplicated cellulitis in diabetic patients. The majority of clinicians (76%) preferred co-amoxiclav, with or without clindamycin, for the treatment of mild to moderate cellulitis in diabetic patients. Around 30% indicated that surgical site infections occur in approximately 11–20% of their patients in routine clinical practice. Most of the clinical experts (81%) identified Staphylococcus aureus as the most common organism responsible for surgical site infections in their clinical practice.
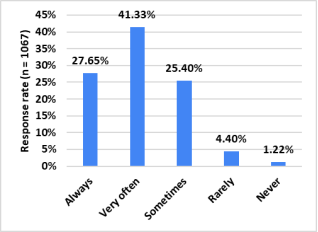
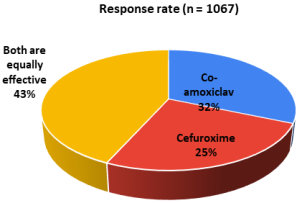
About 41% of experts reported that they very often use cefuroxime as the preferred prophylactic antibiotic in surgical units for minimal access or laparoscopic procedures (Figure 2). Nearly 37% highlighted long-duration sequential prophylaxis as the key advantage of using cefuroxime for surgical prophylaxis in their clinical practice (Table 3). According to 43% of respondents, co-amoxiclav and cefuroxime are equally effective for the management of respiratory tract infections in their clinical practice (Figure 3).
Figure 3. Distribution of responses to perceived effectiveness of antibiotics for respiratory tract infections in clinical practice.
Table 3. Distribution of responses to the advantages of using cefuroxime for surgical prophylaxis in clinical practice.
Reported advantage
Response, N (%)
Single-dose usage
293 (27.46%)
Long-duration sequential prophylaxis
397 (37.21%)
Easy to switch to oral cefuroxime
132 (12.37%)
Cost effective
0 (0%)
All of the above
245 (22.96%)
The predominant proportion of clinicians (66.45%) indicated that bacterial susceptibility is the most important factor guiding their choice between co-amoxiclav and cefuroxime in routine clinical practice (Table 4). A substantial majority (73.29%) reported they had not encountered any adverse drug reactions associated with co-amoxiclav in their clinical practice. Around 46% rated patient outcomes with co-amoxiclav as showing marked improvement on the global improvement scale.
Table 4. Distribution of responses to factors influencing the choice between co-amoxiclav and cefuroxime in clinical practice.
Factors Influencing Antibiotic Choice
N (%)
Bacterial susceptibility
709 (66.45%)
Patient tolerance
138 (12.93%)
Cost-effectiveness
66 (6.19%)
Availability
15 (1.41%)
All of the above
139 (13.03%)
4. Discussion
The survey findings highlight the need for continued surveillance of antimicrobial resistance patterns, reinforcement of antimicrobial stewardship practices, and evidence-based guidance to optimize empiric antibiotic therapy in diverse clinical settings. The data reveal a strong clinician preference for co-amoxiclav across multiple clinical scenarios, while also emphasizing the continued relevance of cefuroxime in surgical prophylaxis settings. The predominance of streptococcal pharyngitis as the most common indication for co-amoxiclav in the present survey is consistent with findings from previous Indian studies evaluating antibiotic usage practices for upper respiratory tract infections. A South Indian study assessing drug-prescribing patterns in acute, recurrent, and chronic pharyngitis reported co-amoxiclav as the most frequently prescribed antibiotic and concluded that it can be considered a mainstay or first-line option because of its well-established efficacy, good tolerability, and relatively low cost. These findings support the widespread clinical reliance on co-amoxiclav for managing bacterial pharyngitis in routine practice.
[9]
Ranabovi D, Ramesh J, Bisanna J, Purushothama PH. A study on the drug prescribing pattern in acute, recurrent and chronic pharyngitis at a tertiary care hospital. International Journal of Basic & Clinical Pharmacology. 2016; 5(4): 1494–8.
Evidence from controlled clinical studies further supports the effectiveness of this agent. A randomized comparative clinical trial conducted by Karpishchenko et al. demonstrated that co-amoxiclav EXPRESS shows high therapeutic efficacy in the treatment of acute streptococcal tonsillopharyngitis, with clinical outcomes comparable to those achieved with conventional Amoxiclav film-coated tablets. The study also reported that the dispersible formulation of co-amoxiclav EXPRESS exhibited a significantly better safety profile compared with the standard tablet formulation, suggesting potential advantages in tolerability and patient adherence.
[10]
Karpishchenko SA, Ryabova MА, Kolesnikova OM, Ulupov MY. [Antibacterial therapy for acute streptococcal tonsillopharyngitis: results of a randomized comparative clinical trial with amoxicillin + clavulanic acid EXPRESS]. Ter Arkh. 2024; 96(3): 273–9.
A high preference for co-amoxiclav as empiric therapy for CAP, both in patients without comorbidities and in those with comorbidities, was observed in the present survey. This finding is consistent with evidence from the Indian literature. A review article from an Indian perspective by Budhiraja et al. reported that co-amoxiclav is among the most commonly prescribed antibiotics, particularly for respiratory tract infections. The review further highlighted that the combination continues to retain its role as a first-line therapy for outpatient CAP because of its broad coverage and sustained sensitivity against commonly implicated respiratory pathogens.
[11]
Budhiraja S, Agarwal A, Chugh Y, Gandhi A, Kotak B. Amoxicillin+clavulanic acid in community acquired pneumonia: Past, present, and future from an Indian perspective. Asian J Med Sci. 2022; 13(8): 235–44.
In addition to respiratory infections, the present survey also demonstrated a strong clinician preference for co-amoxiclav, with or without clindamycin, in the management of mild to moderate diabetic cellulitis. Supporting this observation, Gariani et al. evaluated the effectiveness of co-amoxiclav as an oral therapy for diabetic foot infections and reported a remission rate of 74%. The study concluded that oral co-amoxiclav represents a reasonable and effective treatment option for patients with diabetic foot infections.
[12]
Gariani K, Lebowitz D, Kressmann B, von Dach E, Sendi P, Waibel F, et al. Oral amoxicillin-clavulanate for treating diabetic foot infections. Diabetes Obes Metab. 2019; 21(6): 1483–6.
These findings reinforce the broad clinical utility of co-amoxiclav across multiple community-acquired infections encountered in routine clinical practice.
Regarding surgical prophylaxis, cefuroxime emerged as the preferred prophylactic agent for minimal access and laparoscopic procedures, with the majority of clinicians reporting very frequent use. Additionally, the majority of clinicians highlighted long-duration sequential prophylaxis as the key advantage of cefuroxime. Cephalosporins are widely regarded as the drugs of choice for surgical prophylaxis in general surgery due to their favorable safety profile, potent bactericidal activity, and excellent penetration into critical tissues.
[5]
Sastry GL, Nandi M, Mukhopadhyay M, Dumbre R, Bhattacharjee S, Sukumar G, et al. Role of cefuroxime as antibiotic prophylaxis for general surgery: An expert opinion. IP Journal of Surgery and Allied Sciences. 2025; 3(3): 58–71.
A study by Borade et al. reported that a single preoperative dose of cefuroxime is effective in preventing surgical site infections in elective procedures, provided the surgery is uncomplicated.
[13]
Borade SV, Syed O. Single dose antibiotic prophylaxis for prevention of surgical site infection in elective surgery. International Surgery Journal. 2018; 5(1): 27–33.
The majority of respondents in the present survey perceived co-amoxiclav and cefuroxime to be equally effective for the management of respiratory tract infections. This observation is supported by evidence from comparative clinical studies. A randomized controlled trial by Lari et al., which evaluated the efficacy of cefuroxime and co-amoxiclav in patients with acute sinusitis, reported that twice-daily cefuroxime was comparably effective to thrice-daily co-amoxiclav in achieving clinical improvement.
[14]
Lari AR, Alinejad F, Alaghehbandan R, Mostafavi H, Asghari B, Gholami A. Comparison of cefuroxime and co-amoxiclav in the treatment of acute sinusitis in a sample of the Iranian population. Infez Med. 2012; 20(4): 251–5.
[14]
Similarly, another randomized controlled trial by Pareek et al. assessing treatment outcomes in patients with lower respiratory tract infections demonstrated bacteriological success rates of 95% with cefuroxime–sulbactam and 100% with co-amoxiclav, with no significant difference between the two treatment groups. Both antibiotic regimens were reported to be safe and well tolerated, supporting their comparable clinical effectiveness in respiratory infections.
[15]
Pareek A, Pednekar S, Prasad HB, Salagre S, Chandurkar N. Randomized, multicentre, comparative clinical evaluation of cefuroxime-sulbactam versus amoxicillin-clavulanic acid therapy in the treatment of lower respiratory tract infections. J Int Med Res. 2008; 36(6): 1293–304.
Most clinicians in the survey identified bacterial susceptibility as the most important factor guiding their choice between co-amoxiclav and cefuroxime. This finding reflects an encouraging shift toward evidence-based and susceptibility-guided antibiotic prescribing in routine clinical practice. Antimicrobial susceptibility testing is a laboratory procedure performed by trained medical technologists or clinical laboratory scientists to determine the most effective antimicrobial therapy for individual patients. In addition to guiding patient-level treatment decisions, susceptibility testing plays an important role at institutional and national levels by helping monitor resistance patterns, evaluate treatment practices, and inform strategies aimed at controlling and preventing infectious diseases.
[16]
Bayot ML, Bragg BN. Antimicrobial Susceptibility Testing. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 [cited 2026 Mar 7]. Available from:
The safety profile of co-amoxiclav was viewed favorably, with most clinicians reporting no adverse drug reactions encountered in their clinical practice. The perceived efficacy of co-amoxiclav was reinforced by the finding that the majority of clinicians rated patient outcomes as showing marked improvement, lending further support to its continued role as a preferred empiric agent across multiple infectious indications. A multicenter, real-world study reported that co-amoxiclav demonstrated robust clinical effectiveness and a favorable safety profile in the treatment of dental infections, with the majority of patients achieving complete symptom resolution and a low incidence of adverse events.
[17]
Kumar T, Prakash J, Ahire JS, Pal A, Pawar D, Sharma A. Effectiveness and Safety of Co-Amoxiclav in Dental Infections: A Multicenter, Real-World Study. Annals of Medicine and Medical Sciences. 2025; 4: 670–7.
[17]
Another multicenter, retrospective, real-world study reported that co-amoxiclav demonstrated excellent efficacy and a favorable safety profile in the treatment of upper respiratory tract infections.
[18]
Pal A, Pawar D, Sharma A. Effectiveness of co-amoxiclav in managing upper respiratory tract infections: a multicenter retrospective real-world study. Int J Pharm Clin Res. 2024; 16(11): 928–36.
[18]
The present survey has several strengths, including the large sample size of 1,067 clinicians from across India, which provides a broad overview of antibiotic usage practices in diverse clinical settings. The use of a structured questionnaire enabled the systematic assessment of multiple clinically relevant domains. However, certain limitations should be considered while interpreting the findings. As a questionnaire-based survey, the results rely on self-reported clinician responses and may be subject to recall or response bias. The cross-sectional design reflects clinician perceptions at a single time point and does not establish causal relationships or evaluate actual patient-level clinical outcomes. In addition, the survey did not capture regional variations in resistance patterns, institutional antibiotic policies, or microbiological data, which may influence prescribing behavior.
5. Conclusions
Co-amoxiclav occupies a central position in the empiric management of a broad range of community-acquired infections, including streptococcal pharyngitis, CAP, and diabetic skin and soft tissue infections, across diverse clinical practice settings. Cefuroxime remains a preferred choice for surgical antimicrobial prophylaxis, particularly in laparoscopic procedures, where extended sequential prophylaxis is perceived as a clinical advantage. Clinician decision-making appears to be primarily guided by bacterial susceptibility data, reflecting alignment with antimicrobial stewardship principles. The favorable safety profile and positive patient outcomes associated with co-amoxiclav, as reported by clinicians, further reinforce its utility in routine clinical practice.
Abbreviations
ADRs
Adverse Drug Reactions
CAP
Community-Acquired Pneumonia
FDA
Food and Drug Administration
ICU
Intensive Care Unit
LMICs
Low- and Lower-Middle-Income Countries
LRIs
Lower Respiratory Infections
SSI
Surgical Site Infection
URTIs
Upper Respiratory Tract Infections
Acknowledgments
We would like to thank all the clinicians who participated in this study.
Bhattarai S, Sharma BK, Subedi N, Ranabhat S, Baral MP. Burden of Serious Bacterial Infections and Multidrug-Resistant Organisms in an Adult Population of Nepal: A Comparative Analysis of Minimally Invasive Tissue Sampling Informed Mortality Surveillance of Community and Hospital Deaths. Clin Infect Dis. 2021; 73(Suppl_5): S415–21.
Ram B, Thakur R. Epidemiology and Economic Burden of Continuing Challenge of Infectious Diseases in India: Analysis of Socio-Demographic Differentials. Front Public Health. 2022; 10: 901276.
Jin X, Ren J, Li R, Gao Y, Zhang H, Li J, et al. Global burden of upper respiratory infections in 204 countries and territories, from 1990 to 2019. EClinicalMedicine. 2021; 37: 100986.
GBD 2021 Lower Respiratory Infections and Antimicrobial Resistance Collaborators. Global, regional, and national incidence and mortality burden of non-COVID-19 lower respiratory infections and aetiologies, 1990-2021: a systematic analysis from the Global Burden of Disease Study 2021. Lancet Infect Dis. 2024; 24(9): 974–1002.
Sastry GL, Nandi M, Mukhopadhyay M, Dumbre R, Bhattacharjee S, Sukumar G, et al. Role of cefuroxime as antibiotic prophylaxis for general surgery: An expert opinion. IP Journal of Surgery and Allied Sciences. 2025; 3(3): 58–71.
Jena D, Kanti Ghosh T, Pal A, Pawar D, Sharma A. Exploring the Therapeutic Potential of High Dose Co-amoxiclav (1 gm) in Different Clinical Conditions: A Review. Cureus. 2024; 16(7): e64717.
Choudhury J, Makkar A, Sharma V, Karamath SP, Parmar V, Kumar J P, et al. A Real-World Perspective of Co-amoxiclav Prescription Pattern with Probiotics for Pediatric Patients with Respiratory Tract Infections: Results of Quantitative and Qualitative Approach in Indian Outpatient Settings. Cureus. 2023; 15(3): e36269.
Ranabovi D, Ramesh J, Bisanna J, Purushothama PH. A study on the drug prescribing pattern in acute, recurrent and chronic pharyngitis at a tertiary care hospital. International Journal of Basic & Clinical Pharmacology. 2016; 5(4): 1494–8.
Karpishchenko SA, Ryabova MА, Kolesnikova OM, Ulupov MY. [Antibacterial therapy for acute streptococcal tonsillopharyngitis: results of a randomized comparative clinical trial with amoxicillin + clavulanic acid EXPRESS]. Ter Arkh. 2024; 96(3): 273–9.
Budhiraja S, Agarwal A, Chugh Y, Gandhi A, Kotak B. Amoxicillin+clavulanic acid in community acquired pneumonia: Past, present, and future from an Indian perspective. Asian J Med Sci. 2022; 13(8): 235–44.
Borade SV, Syed O. Single dose antibiotic prophylaxis for prevention of surgical site infection in elective surgery. International Surgery Journal. 2018; 5(1): 27–33.
Lari AR, Alinejad F, Alaghehbandan R, Mostafavi H, Asghari B, Gholami A. Comparison of cefuroxime and co-amoxiclav in the treatment of acute sinusitis in a sample of the Iranian population. Infez Med. 2012; 20(4): 251–5.
[15]
Pareek A, Pednekar S, Prasad HB, Salagre S, Chandurkar N. Randomized, multicentre, comparative clinical evaluation of cefuroxime-sulbactam versus amoxicillin-clavulanic acid therapy in the treatment of lower respiratory tract infections. J Int Med Res. 2008; 36(6): 1293–304.
Kumar T, Prakash J, Ahire JS, Pal A, Pawar D, Sharma A. Effectiveness and Safety of Co-Amoxiclav in Dental Infections: A Multicenter, Real-World Study. Annals of Medicine and Medical Sciences. 2025; 4: 670–7.
[18]
Pal A, Pawar D, Sharma A. Effectiveness of co-amoxiclav in managing upper respiratory tract infections: a multicenter retrospective real-world study. Int J Pharm Clin Res. 2024; 16(11): 928–36.
Suresh, M., Manjunath, K. K. (2026). Expert Perspectives on the Usage of Co-amoxiclav and Cefuroxime in Clinical Practice: A Cross-Sectional Survey from Indian Settings. International Journal of Infectious Diseases and Therapy, 11(2), 23-29. https://doi.org/10.11648/j.ijidt.20261102.12
Suresh, M.; Manjunath, K. K. Expert Perspectives on the Usage of Co-amoxiclav and Cefuroxime in Clinical Practice: A Cross-Sectional Survey from Indian Settings. Int. J. Infect. Dis. Ther.2026, 11(2), 23-29. doi: 10.11648/j.ijidt.20261102.12
Suresh M, Manjunath KK. Expert Perspectives on the Usage of Co-amoxiclav and Cefuroxime in Clinical Practice: A Cross-Sectional Survey from Indian Settings. Int J Infect Dis Ther. 2026;11(2):23-29. doi: 10.11648/j.ijidt.20261102.12
@article{10.11648/j.ijidt.20261102.12,
author = {Manjula Suresh and Krishna Kumar Manjunath},
title = {Expert Perspectives on the Usage of Co-amoxiclav and Cefuroxime in Clinical Practice: A Cross-Sectional Survey from Indian Settings},
journal = {International Journal of Infectious Diseases and Therapy},
volume = {11},
number = {2},
pages = {23-29},
doi = {10.11648/j.ijidt.20261102.12},
url = {https://doi.org/10.11648/j.ijidt.20261102.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijidt.20261102.12},
abstract = {Background: Although there are several clinical studies available regarding the management of bacterial infections, there is a dearth of studies among clinical experts on their practice. The survey aimed to assess clinical preferences and decision-making factors among clinicians regarding the use of co-amoxiclav and cefuroxime across a range of common infections and surgical indications in routine clinical practice in Indian settings. Methodology: This cross-sectional study was conducted among clinicians across India using a 22-item structured questionnaire. The questionnaire assessed common infection types, antibiotic usage patterns, indications for co-amoxiclav and cefuroxime, preferred regimens for community-acquired pneumonia (CAP), skin and soft tissue infections, and surgical prophylaxis, perceived comparative efficacy, factors influencing antibiotic choice, adverse drug reactions, and clinical outcomes using a global improvement scale. The data were analyzed using descriptive statistics. Results: Approximately 49% of clinicians identified streptococcal pharyngitis as the most common indication for recommending co-amoxiclav in routine practice. Nearly 60% reported co-amoxiclav as the most preferred empiric antimicrobial therapy for adult CAP in patients without comorbidities, while about 51% preferred it in patients with comorbidities. Around 76% of clinicians favored co-amoxiclav, with or without clindamycin, for the management of mild to moderate cellulitis in diabetic patients. Approximately 41% reported cefuroxime as the preferred prophylactic antibiotic for minimal access or laparoscopic surgeries, and about 37% highlighted long-duration sequential prophylaxis as its key advantage. Nearly 43% of respondents considered co-amoxiclav and cefuroxime to be equally effective for respiratory tract infections. About 66% of clinicians identified bacterial susceptibility as the most important factor influencing the choice between co-amoxiclav and cefuroxime. Conclusion: Co-amoxiclav is the preferred empiric antibiotic for streptococcal pharyngitis, CAP, and diabetic cellulitis, while cefuroxime remains the agent of choice for surgical prophylaxis in laparoscopic procedures. Bacterial susceptibility is the primary factor guiding antibiotic selection. The favorable safety profile and positive patient outcomes associated with co-amoxiclav support its continued role as a cornerstone agent in the empiric management of community-acquired infections in routine clinical practice.},
year = {2026}
}
TY - JOUR
T1 - Expert Perspectives on the Usage of Co-amoxiclav and Cefuroxime in Clinical Practice: A Cross-Sectional Survey from Indian Settings
AU - Manjula Suresh
AU - Krishna Kumar Manjunath
Y1 - 2026/06/25
PY - 2026
N1 - https://doi.org/10.11648/j.ijidt.20261102.12
DO - 10.11648/j.ijidt.20261102.12
T2 - International Journal of Infectious Diseases and Therapy
JF - International Journal of Infectious Diseases and Therapy
JO - International Journal of Infectious Diseases and Therapy
SP - 23
EP - 29
PB - Science Publishing Group
SN - 2578-966X
UR - https://doi.org/10.11648/j.ijidt.20261102.12
AB - Background: Although there are several clinical studies available regarding the management of bacterial infections, there is a dearth of studies among clinical experts on their practice. The survey aimed to assess clinical preferences and decision-making factors among clinicians regarding the use of co-amoxiclav and cefuroxime across a range of common infections and surgical indications in routine clinical practice in Indian settings. Methodology: This cross-sectional study was conducted among clinicians across India using a 22-item structured questionnaire. The questionnaire assessed common infection types, antibiotic usage patterns, indications for co-amoxiclav and cefuroxime, preferred regimens for community-acquired pneumonia (CAP), skin and soft tissue infections, and surgical prophylaxis, perceived comparative efficacy, factors influencing antibiotic choice, adverse drug reactions, and clinical outcomes using a global improvement scale. The data were analyzed using descriptive statistics. Results: Approximately 49% of clinicians identified streptococcal pharyngitis as the most common indication for recommending co-amoxiclav in routine practice. Nearly 60% reported co-amoxiclav as the most preferred empiric antimicrobial therapy for adult CAP in patients without comorbidities, while about 51% preferred it in patients with comorbidities. Around 76% of clinicians favored co-amoxiclav, with or without clindamycin, for the management of mild to moderate cellulitis in diabetic patients. Approximately 41% reported cefuroxime as the preferred prophylactic antibiotic for minimal access or laparoscopic surgeries, and about 37% highlighted long-duration sequential prophylaxis as its key advantage. Nearly 43% of respondents considered co-amoxiclav and cefuroxime to be equally effective for respiratory tract infections. About 66% of clinicians identified bacterial susceptibility as the most important factor influencing the choice between co-amoxiclav and cefuroxime. Conclusion: Co-amoxiclav is the preferred empiric antibiotic for streptococcal pharyngitis, CAP, and diabetic cellulitis, while cefuroxime remains the agent of choice for surgical prophylaxis in laparoscopic procedures. Bacterial susceptibility is the primary factor guiding antibiotic selection. The favorable safety profile and positive patient outcomes associated with co-amoxiclav support its continued role as a cornerstone agent in the empiric management of community-acquired infections in routine clinical practice.
VL - 11
IS - 2
ER -
Suresh, M., Manjunath, K. K. (2026). Expert Perspectives on the Usage of Co-amoxiclav and Cefuroxime in Clinical Practice: A Cross-Sectional Survey from Indian Settings. International Journal of Infectious Diseases and Therapy, 11(2), 23-29. https://doi.org/10.11648/j.ijidt.20261102.12
Suresh, M.; Manjunath, K. K. Expert Perspectives on the Usage of Co-amoxiclav and Cefuroxime in Clinical Practice: A Cross-Sectional Survey from Indian Settings. Int. J. Infect. Dis. Ther.2026, 11(2), 23-29. doi: 10.11648/j.ijidt.20261102.12
Suresh M, Manjunath KK. Expert Perspectives on the Usage of Co-amoxiclav and Cefuroxime in Clinical Practice: A Cross-Sectional Survey from Indian Settings. Int J Infect Dis Ther. 2026;11(2):23-29. doi: 10.11648/j.ijidt.20261102.12
@article{10.11648/j.ijidt.20261102.12,
author = {Manjula Suresh and Krishna Kumar Manjunath},
title = {Expert Perspectives on the Usage of Co-amoxiclav and Cefuroxime in Clinical Practice: A Cross-Sectional Survey from Indian Settings},
journal = {International Journal of Infectious Diseases and Therapy},
volume = {11},
number = {2},
pages = {23-29},
doi = {10.11648/j.ijidt.20261102.12},
url = {https://doi.org/10.11648/j.ijidt.20261102.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijidt.20261102.12},
abstract = {Background: Although there are several clinical studies available regarding the management of bacterial infections, there is a dearth of studies among clinical experts on their practice. The survey aimed to assess clinical preferences and decision-making factors among clinicians regarding the use of co-amoxiclav and cefuroxime across a range of common infections and surgical indications in routine clinical practice in Indian settings. Methodology: This cross-sectional study was conducted among clinicians across India using a 22-item structured questionnaire. The questionnaire assessed common infection types, antibiotic usage patterns, indications for co-amoxiclav and cefuroxime, preferred regimens for community-acquired pneumonia (CAP), skin and soft tissue infections, and surgical prophylaxis, perceived comparative efficacy, factors influencing antibiotic choice, adverse drug reactions, and clinical outcomes using a global improvement scale. The data were analyzed using descriptive statistics. Results: Approximately 49% of clinicians identified streptococcal pharyngitis as the most common indication for recommending co-amoxiclav in routine practice. Nearly 60% reported co-amoxiclav as the most preferred empiric antimicrobial therapy for adult CAP in patients without comorbidities, while about 51% preferred it in patients with comorbidities. Around 76% of clinicians favored co-amoxiclav, with or without clindamycin, for the management of mild to moderate cellulitis in diabetic patients. Approximately 41% reported cefuroxime as the preferred prophylactic antibiotic for minimal access or laparoscopic surgeries, and about 37% highlighted long-duration sequential prophylaxis as its key advantage. Nearly 43% of respondents considered co-amoxiclav and cefuroxime to be equally effective for respiratory tract infections. About 66% of clinicians identified bacterial susceptibility as the most important factor influencing the choice between co-amoxiclav and cefuroxime. Conclusion: Co-amoxiclav is the preferred empiric antibiotic for streptococcal pharyngitis, CAP, and diabetic cellulitis, while cefuroxime remains the agent of choice for surgical prophylaxis in laparoscopic procedures. Bacterial susceptibility is the primary factor guiding antibiotic selection. The favorable safety profile and positive patient outcomes associated with co-amoxiclav support its continued role as a cornerstone agent in the empiric management of community-acquired infections in routine clinical practice.},
year = {2026}
}
TY - JOUR
T1 - Expert Perspectives on the Usage of Co-amoxiclav and Cefuroxime in Clinical Practice: A Cross-Sectional Survey from Indian Settings
AU - Manjula Suresh
AU - Krishna Kumar Manjunath
Y1 - 2026/06/25
PY - 2026
N1 - https://doi.org/10.11648/j.ijidt.20261102.12
DO - 10.11648/j.ijidt.20261102.12
T2 - International Journal of Infectious Diseases and Therapy
JF - International Journal of Infectious Diseases and Therapy
JO - International Journal of Infectious Diseases and Therapy
SP - 23
EP - 29
PB - Science Publishing Group
SN - 2578-966X
UR - https://doi.org/10.11648/j.ijidt.20261102.12
AB - Background: Although there are several clinical studies available regarding the management of bacterial infections, there is a dearth of studies among clinical experts on their practice. The survey aimed to assess clinical preferences and decision-making factors among clinicians regarding the use of co-amoxiclav and cefuroxime across a range of common infections and surgical indications in routine clinical practice in Indian settings. Methodology: This cross-sectional study was conducted among clinicians across India using a 22-item structured questionnaire. The questionnaire assessed common infection types, antibiotic usage patterns, indications for co-amoxiclav and cefuroxime, preferred regimens for community-acquired pneumonia (CAP), skin and soft tissue infections, and surgical prophylaxis, perceived comparative efficacy, factors influencing antibiotic choice, adverse drug reactions, and clinical outcomes using a global improvement scale. The data were analyzed using descriptive statistics. Results: Approximately 49% of clinicians identified streptococcal pharyngitis as the most common indication for recommending co-amoxiclav in routine practice. Nearly 60% reported co-amoxiclav as the most preferred empiric antimicrobial therapy for adult CAP in patients without comorbidities, while about 51% preferred it in patients with comorbidities. Around 76% of clinicians favored co-amoxiclav, with or without clindamycin, for the management of mild to moderate cellulitis in diabetic patients. Approximately 41% reported cefuroxime as the preferred prophylactic antibiotic for minimal access or laparoscopic surgeries, and about 37% highlighted long-duration sequential prophylaxis as its key advantage. Nearly 43% of respondents considered co-amoxiclav and cefuroxime to be equally effective for respiratory tract infections. About 66% of clinicians identified bacterial susceptibility as the most important factor influencing the choice between co-amoxiclav and cefuroxime. Conclusion: Co-amoxiclav is the preferred empiric antibiotic for streptococcal pharyngitis, CAP, and diabetic cellulitis, while cefuroxime remains the agent of choice for surgical prophylaxis in laparoscopic procedures. Bacterial susceptibility is the primary factor guiding antibiotic selection. The favorable safety profile and positive patient outcomes associated with co-amoxiclav support its continued role as a cornerstone agent in the empiric management of community-acquired infections in routine clinical practice.
VL - 11
IS - 2
ER -